Function
The Common Vein Copyright 2007
Transport function
The contents of the colon move in a slow and steady fashion. If the colon were to be an instrument in a band or an orchestra I would imagine it would be in the bass or double bass section. Its nature is quiet, efficient, deep, slow, and essential. It gets the job done without drama and fanfare. Occasionally it does have to let off some steam in which case it brings in the wind instruments and changes its pitch, but most of the day and night it is droning away, working slowly and efficiently in the background. It may take several days for stool to move from the cecum to the rectum. Movement of the colon is complex in the variety of contraction patterns which are executed by an inner circular and outer longitudinal muscle. The contractions result in two basic patterns – one optimized for mixing and the other for propulsion. Tonic contractions of these muscles result in a mixing pattern of the stool while rhythmic contractions serve to propel the stool. Borborygmi is the fancy name given to the gurgling or rumbling sound made by the gastrointestinal tract as it moves water and gas over each other. These sounds are not specific to the colon and originate in the stomach, small intestine and colon. They usually start at low pitch and end after about 30 seconds at a higher pitch. In patients with intestinal obstruction these sounds become exaggerated in intensity and frequency as a result of the attempt of the bowel to push its contents along. As the muscle tires late in the process the sounds may become ominously quiet in bowel obstruction.
Muscles of the colon
The location of the smooth muscle of the large bowel is consistent with other tubular systems of the body since it is found in the muscularis layer between the submucosa and the outer serosa or adventitia. The inner circular muscle has classical arrangement in that it is found in almost uniform thickness surrounding the entire large bowel. The longitudinal muscle concentrates and thickens in three longitudinal muscle bands as noted previously called taenia coli, each about 6-8mms in width. They run almost the entire length of the colon, only becoming more uniform and forming a continuous, complete, circumferential layer at the level of the rectum. They are unique to the colon and are located at equal distances from each other around the circumference of the colon.
The presence of the longitudinal muscles along three fixed points of the colon creates a pleating effect and creates the haustra or sacs which facilitate storage and to some extent increase the surface area of the colon. (a haustrum is the singular form of haustra) On the luminal side the pleating effects causes folds in the mucosa called plica circulares or semilunar folds. When the contraction of the taenia is strong the haustral pattern is marked and when they relax the haustral pattern may be absent. If the taenia were to be removed from the colon it would be a longer and straighter organ without its haustrations.
Sometimes when the ascending colon is cut perfectly transversely on a CT scan, and because the taenia are equidistant and the degree of contraction is perfect, the haustra produce a perfect clover leaf formation.
|
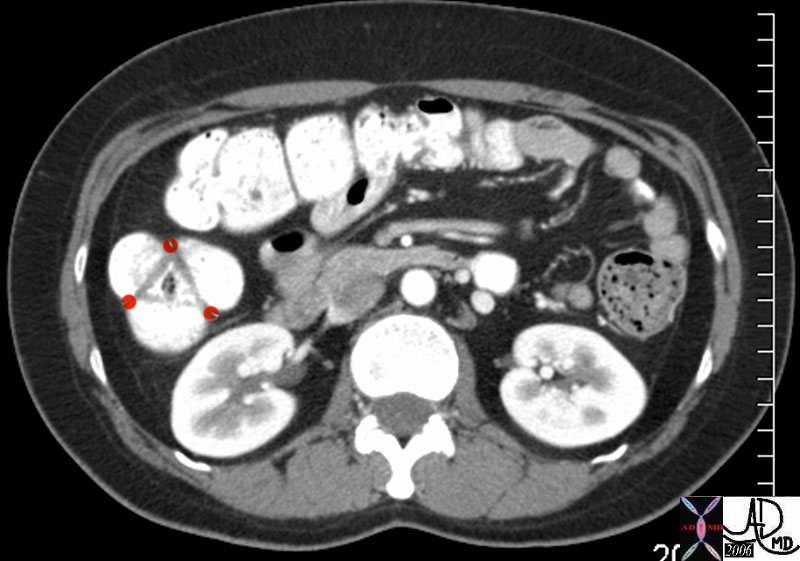
| When the ascending colon is cut perfectly transversely, the three equidistant haustra produce a shape that looks like a clover leaf. The taenia are positioned at each point of the infolding. These muscle bands are relatively flat and so are not usually seen radiologically. The anterior taenia of the ascending colon is the taenia libera, while the medial muscle is the taenia mesocolica, and the lateral bundle is called the taenia omentalis. The triangle that is seen in this image represent the plica circulares which are the mucosal folds seen on the luminal side caused by the pleating effect discussed above.
Courtesy Ashley Davidoff MD 45209b01 74664p |
 Tenia coli – a perfect clover leaf
Tenia coli – a perfect clover leaf
The circular muscles in addition undergo focal areas of intermittent tonic contractions, which are about 2.5cms wide, causing slight indentations within the haustra while the intervening bowel and smooth muscle relax. These contractions last about 30 seconds and they cause the chyme and evolving stool to be compressed and churned within the haustra. Once a particular band relaxes a band in another region repeats the contraction so that contents within an haustration gets churned and compressed. These circular contractions are particularly prominent on the right side of the colon where mixing and churning are the dominant function allowing more stool to be exposed to the mucosa so that water and electrolytes can be absorbed.
 Feces in the haustra Feces in the haustra |
| The barium coated feces is seen within the haustra taking on the shape of the haustra. The stool remains in the haustra for sometime during which muscle contractions compress and mould the feces into its own shape.
Courtesy Ashley Davidoff MD 45663 |
  Tonic contraction in the rectosigmoid Tonic contraction in the rectosigmoid |
| These images reflect a contraction band in the rectosigmoid region.. The colon upstream of the contraction I relaxed as is the colon that is distal to the contraction.
Courtesy Ashley Davidoff MD 45441 45441b01 |
 Propulsive movement Propulsive movement |
| Note the two long regions of peristalsis in the entire transverse colon and proximal portion in the descending colon in this 95 year old male. Other observations include the remarkable absence of diverticulosis, and the redundancy of both the hepatic flexure and the splenic flexure.
Courtesy Ashley Davidoff MD 45660 |
The non propulsive movements described above are intermittently combined with propulsive movements including slow irregular contractions that are more rhythmic in their nature. There is one type of propulsive movement which serves to slowly edge the stool forward caused by a contraction wave that starts proximally, is short lived, and involves a relatively short segment of colon. The second type of propulsive movement is stronger, occurs a few times in the day, and results in a mass movement where the product is aggressively moved onward and forward and when the colon shows off its muscular strength and power. This function is also called mass peristalsis, and most commonly occurs after a meal induced by the gastrocolic and duodenocolic reflexes. This type of propulsive movement is also stimulated when a person wakes in the morning. Propulsive movements allow emptying of the upstream bowel of relatively large amounts of stool. The stool is moved a relatively long distance, and provides room for incoming contents. As stool moves downstream the function of the colon evolves from churning and mixing to one of storage. There is also a pattern of muscular function called receptive relaxation which enables the receiving part of the bowel to accommodate new volume of chyme or stool. The movement of the stool is almost factory like with the product on a conveyer belt being worked on, refined and produced in the initial stages and when ready, signaled to move on where it is stored until it can be mailed out to its final destination.
Thus the smooth muscle of the gastrointestinal tract is designed to allow a coordinated and connected contractile movement. The individual cells are connected through their cell membranes in an intimate fashion to each other, allowing the cells to behave as a syncitium. This means that muscle activity in one muscle fiber is easily transmitted and propagated to other muscle fibers. This close connection allows for transmission of electrical activity through the muscle – usually a function restricted to the nerves. In the colon therefore, muscle movement is controlled through both the usual autonomic innervation, hormonal control, as well as through muscle activity itself.
Evacuation or defecation
The mechanisms involved with defecation are even more complex since they involve somatic and visceral nerves, voluntary and involuntary muscles, and cerebral and an autonomic nervous system control. When the rectum fills, the person becomes conscious of a need to evacuate. The sensory path is so beautifully adapted enabling exquisite differentiation by pressure sensors to be made between air, watery stool, and solid stool. Even our second set of eyes (our hands) cannot easily “feel” air. Have you ever been able to hold a volume of air in your hand and sense its presence? Of course if the air is moving or under pressure you will, but the sensory powers of the rectum and stomach in particular, and the gastrointestinal tract in general, are quite outstanding in their ability to sense gaseous content.
Once rectal fullness is sensed it is left up to cerebral decisions as to when emptying will take place. In health the rectum should be empty since the function of the rectum is really to sense the presence of contents, discriminate the type of content, and then in the best of worlds to evacuate contents as soon as possible. The rectum is a type of post office – once the letters and parcels come in they should be transported to their destinations as soon as possible – do not allow backup! Since there is such a strong cerebral component to evacuation and since it is often not convenient, we often postpone the inevitable, and override the urge in our busy lives. Sometimes this may cause retroperistalsis which empties the rectum back to the sigmoid and quells the urge. If we postpone evacuation too frequently and for too long, the rectum becomes stretched and or the sensory fibers adapt, and our sensors sour and become less effective. The full rectum and the impacted rectum (rectum fa-shtoptum – a Yiddish phrase from the old country) is an entity seen in the pediatric population and even more so in the aging, the aged, the infirm, and the mentally handicapped.
There are two sphincters surrounding the rectum and the anal canal and a group of muscles called the levator ani muscles which are all functionally related to enable defecation. The internal sphincter is controlled by the autonomic nervous system and the external sphincter and levator ani by voluntary mechanisms. Once the decision to evacuate is made, the person will open the external sphincter and the internal sphincter will open in sympathy resulting in strong propulsive peristaltic wave, usually aided by a Valsalva maneuver allowing contents to move into the free world. This can occur normally from as frequently as several times in a day to as infrequently as once every few days.
 The empty rectal vault The empty rectal vault |
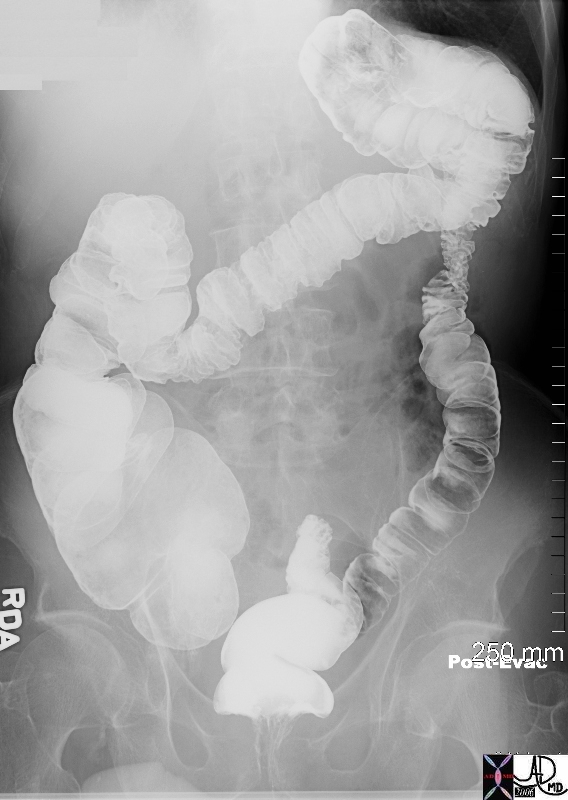
| The single contrast barium enema has been followed by a post evacuation film. It shows an empty rectal vault and heaping up of the proximal ampulla on the distal ampulla presumably due to the contraction of the puborectalis and external sphincter.
Courtesy Ashley Davidoff MD
45661 |
 Post evacuation CT Post evacuation CT |
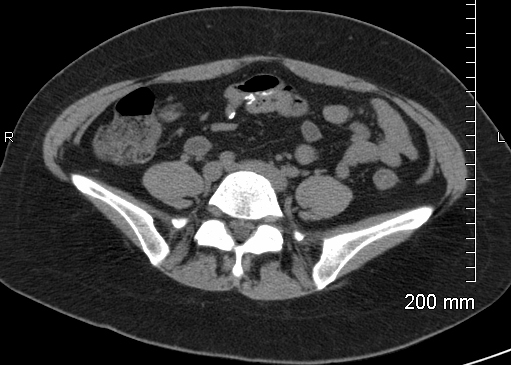
| Post evacuation CT image on the right shows an ascending colon with semi solid stool characterized by an air fluid level, and a descending colon that is empty. The colon frames the abdomen so that the ascending colon I the most rightward structure while on the left it is posterolateral. The sigmoid colon and rectum are also empty as seen in he second image. The patient defecated just before the scan was performed
45198 45201 Courtesy Ashley Davidoff MD |
|
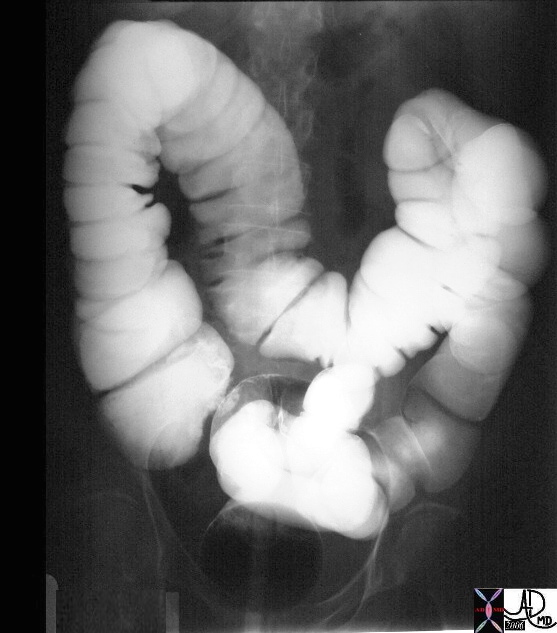
| This series of two images shows the efficiency of the evacuation process. The image on the right is from a single contrast barium enema showing a colon distended with contrast, followed by the post evacuation film which shows about 80 percent of barium was evacuated. Note that a small amount of barium refluxed into the terminal ileum on the “post evac”, that the cecum, ascending transverse and part of descending colon are decompressed, and that the distal descending, and sigmoid colon are entirely empty while the rectum has a small residual within it. Now that is what you call a bowel movement! Some people would die for this kind of result.
Courtesy Ashley Davidoff MD 28693 28695 |
 Pre and post evacuation barium study
Pre and post evacuation barium studyAbsorptive function
On the average about 1.5 liters of fluid enter the colon and only about 100-200ccs is excreted in the stool so that 90-95% of the water is reabsorbed. The maximum absorptive power of the colon is about 4.5 liters per day. In disease states where more than 4.5 liters is presented, diarrhea will result.
Most of the absorption takes place in the ascending colon with the descending colon acting in storage capacity. Electrolytes and particularly sodium are absorbed by the creation of a gradient by the sodium pump, which also helps in the absorption of water. There is active secretion of bicarbonate which helps neutralize the acid produced by the bacteria.
  Moving chyme into the cecum Moving chyme into the cecum |
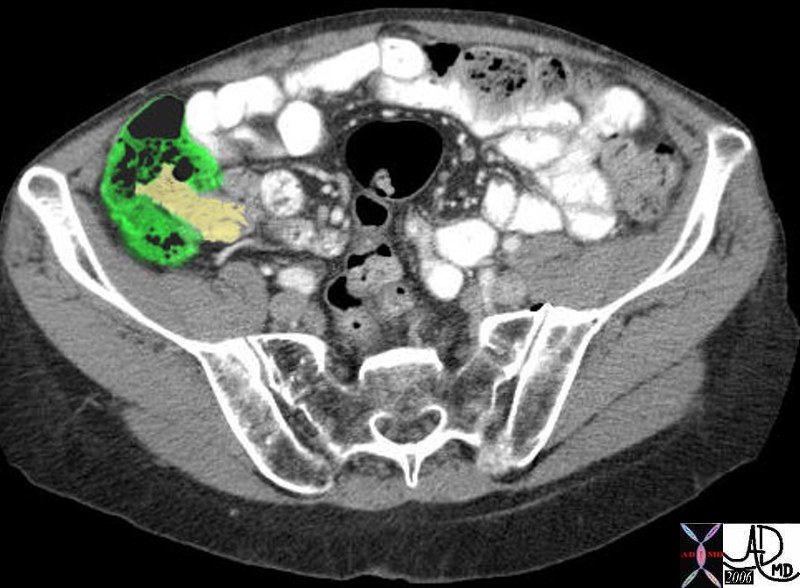
| In these two images we note the terminal ileum (overlay yellow) presenting fluid contents to the cecum (overlay in green) The main absorptive function of the colon is to preserve as much of the water as possible and to absorb any useful nutrients that can be recovered and recycled.
Courtesy Ashley Davidoff MD 37819 37819b01 |
Digestion and Absorption of Undigested Food Products
The colon is filled with an abundant zoo of anaerobic and aerobic bacteria which for the health of the body have to be caged in the “safe” environment of the colon since if let loose into the rest of the body can be lethal foes. Thereare over 400 species of organisms that live in the colon including bacteria yeasts and some parasites. Most of these function as ferementers and are helpful, some are just there for the ride providing no significant contribution, while others have the potential to be harmful. Other than functioning to ferment complex carbohydrates, they also synthesize vitamins like B12, biotin, thiamin, riboflavin and vitamin K. Vitamin K is especially impotrant . Lactobacillus Acidophilus provides an antibacterial activity against many potentially harmful gram-negative and gram-positive pathogens.
The anaerobic bacteria dominate in the large bowel and together with the aerobic bacteria help break down and ferment products that were either missed by the small bowel or that were incapable of digestion by the small bowel such as cellulose and other complex carbohydrates found in fiber. Small amounts of fat starch and proteins are also digested by these colonic mechanisms. E Coli can for example help split triglycerides. A small amount of complex carbohydrates are thus broken down into short chain fatty acids which are easily absorbed by colonic mucosa. The amount of energy provided by this process however is very small.
The human body lacks the enzyme called alpha-galactosidase that is required for the digestion of the complex carbohydrates found in vegetables such as beans, cabbage, soybeans, broccoli peas and onions. Beans contain particularly large amounts of complex carbohydrates and hence their notoriety as gas producers. Complex sugars are fermented by the bacteria, forming the short-chain fatty acids, butyrate, propionate and acetate. The fermentation process produces gas that contains hydrogen, carbon dioxide, and methane which are found both within the stool and in the lumen of the colon. Some people are unable to digest simpler sugars in the small bowel such as lactose which is found in milk and other dairy products. These simpler sugars are therefore presented to the large bowel where the fermenters turn the sugars into gas. When excessive gas is produced in these patients, symptoms include abdominal pain, discomfort bloating and flatulence.
The gas produced by the fermentation process can be found either within the stool or within the lumen of the bowel. If there is excessive gas within the stool it floats because the specific gravity is less than water. It is the gas that is in the lumen that causes distension of the bowel, which in turn stimulates the pressure sensing nerves in the wall of the bowel and in turn the sensation of flatulence. If the gas is upstream in the colon it may cause discomfort and pain and if it is downstream near the sigmoid colon and rectum a stimulus is created and interpreted as “gas waiting to be passed” and it can be passed on a voluntary basis.
 Types of colonic contents Types of colonic contents |
| In this patient three forms of colonic content are identified. The feces labeled ‘A” is classical solid feces dominated by solid material with bubbles of air mixed within. “B” represents a lumen filled with pure air, while “C” is solid stool that has air as its dominant pattern. It is this type of stool that will be a floater in the toilet pan.
Courtesy Ashley Davidoff MD 45328b01 |
 Free air and trapped air Free air and trapped air |
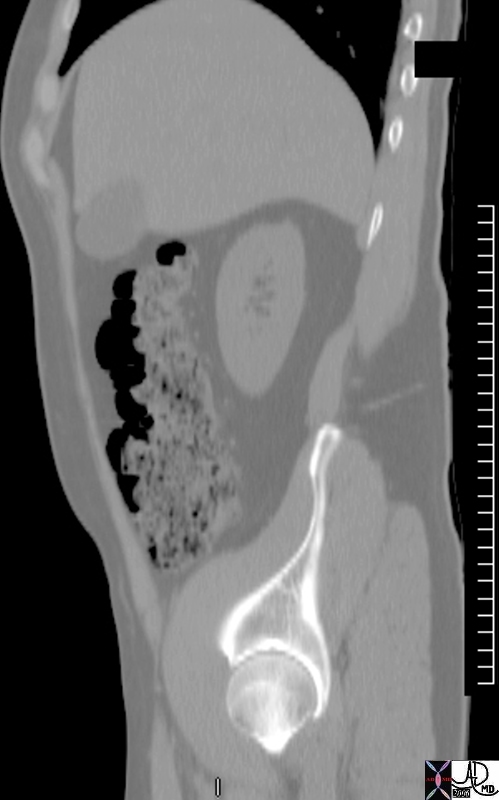
| This sagittal reformat with the patient in the supine position allows free gas to float to the anterior aspect of the colon while air produced in the feces is trapped as small bubbles.
Courtesy Ashley Davidoff MD 45443 |
Mucus secretion
In the depths of the crypts of Lieberkuhn, mucus secreting cells called goblet cells are abundant. There are no enzyme secreting cells in these pits of the large bowel. Mucus is a normal secretion that is an excellent lubricant and protectant. It is spread on the surface of the bowel as a thin film preventing direct contact of the feces on the mucosa and thus protecting the mucosa from mechanical injury. It also adheres to the feces which enables the fecal nuggets (aka scybalae) to adhere to each other forming a stool mass which in turn facilitates transport. The mucus on the surface results in reduced friction of the feces and additionally helps transport of the stool. The mucus acts as a mechanical barrier to the zoo of bacteria that are housed in the colon and with an alkaline PH of about 8 it neutralizes acids in the stool. When the colonic wall becomes irritated, colitis – an inflammation of the wall results, causing the mucosa to exude and secrete water, elecrolytes and mucus. In addition, mucosal dysfunction in colitis will also prevent water that is arriving from the small bowel not to be optimally absorbed. The clinical consequence is a watery diarrhea, often with mucus. If severe enough and left untreated dehydration can ensue, which in the young and elderly can be fatal.