Colon Carcinoma
The Common Vein Copyright 2008
Definition
Colon carcinoma is a malignant disease and is characterized by insidious but progressive nature and late clinical presentation.
It is the second most common cancer and cause of cancer deaths in the United States.
The disease has multifactorial causes with the most common cause having no single known specific etiological factor. The strongest causative link relates to patients with familial adenomatous polyposis. 100% of patients with this entity will develop carcinoma of the colon and a large percentage of patients with longstanding ulcerative colitis will develop carcinoma as well. It is therefore imperative that these patients undergo colectomies before the risk of carcinoma becomes a reality.
As a malignant epithelial tumor in a capacious organ the clues to its presence are few in the early stages of the disease. The earliest clinical clue in the unsuspected patient is the presence of blood in the stool (hemoccult test) or the presence of anemia.
The neoplastic proliferation usually starts out as an adenomatous polyp and progresses over many years resulting in a clinical or pathological feature
Complications include systemic and local metastatic disease, obstruction and perforation.
The diagnosis is suspected clinically in middle aged or elderly patients who are anemic or who have guiaic positive stools and it is confirmed by colonoscopy with biopsy.
If detected early, colorectal cancer is curable by surgery.
Imaging includes the use of endoscopy, barium enema and CTcolonography.
Treatment options depend on the staging of the disease but include surgery, systemic and locoregional chemotherapy Adjuvant chemotherapy can prolong survival in disease that has reached the lymph nodes. Radiotherapy is used in cases of rectal cancer to reduce local recurrence.
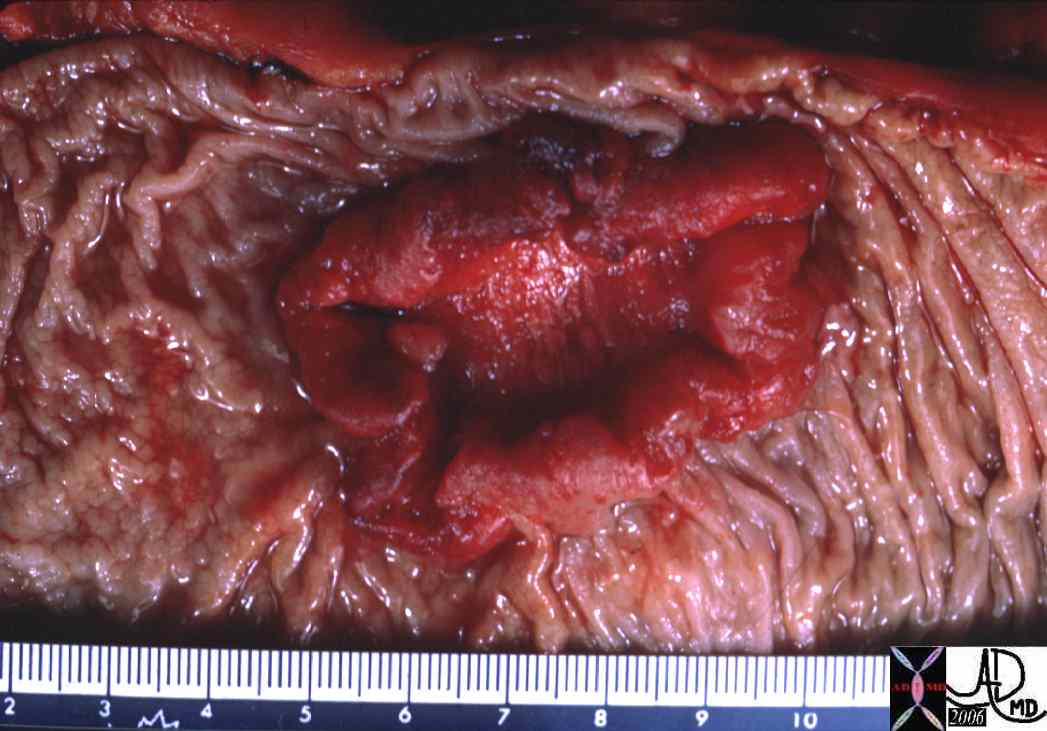 Ulcerating Colon Carcinoma Ulcerating Colon Carcinoma |
| This specimen has obvious malignant characteristics macroscopically, characterized by heaped edges and central ulceration.
Note 02499 colon large bowel fx mass fx ulcerating mass fx raised edges fx central necrosis dx carcinoma malignant primary tumor cancer grosspathology Courtesy Dr Gutkin MD |
Principles
The mucosa is a metabolically active structure with rapid turnover. Intermittantly new cells with either spontaneous mutation or mutations as a result of an environmental pathogen or carcinogen, proliferate. Malignant growth is characterized by unrelenting expansion of the malignant cell population without regard for the organism. When the malignant growth arises from an epithelium it develops into a carcinoma, and when it arises from stromal tissue it becomes a sarcoma. Since the mucosa of the colon has glandular elements the carcinoma arising from the colon is called an adenocarcinoma. The colonic mucosa also secretes mucin and so histopathologically entity may present as a mucinous adenocarcinoma.
The colon is a capacious tube and the tumor is usually far advanced before the transport function becomes impeded. Thus obstruction is a late manifestation. because of the occult nature of the disease diagnostic endeavours are focused on screening for early detection to enable the chance for prevention and cure.
Principles of Disease
Most colorectal cancers are adenocarcinomas, which arise from preexisting adenomatous polyps that develop in the normal colonic mucosa. There is a well recognized adenoma-carcinoma sequence. The most common site for tumor development is the mucosa. The mucosa is a highly active structure and cell turnover is rapid, with the reproduction of new cells and death of old cells occurring about every four days.
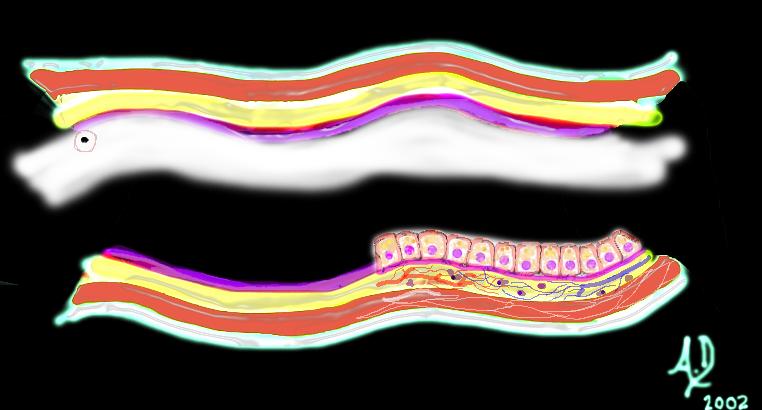 Mucosal disease –beginning of a neoplasm Mucosal disease –beginning of a neoplasm |
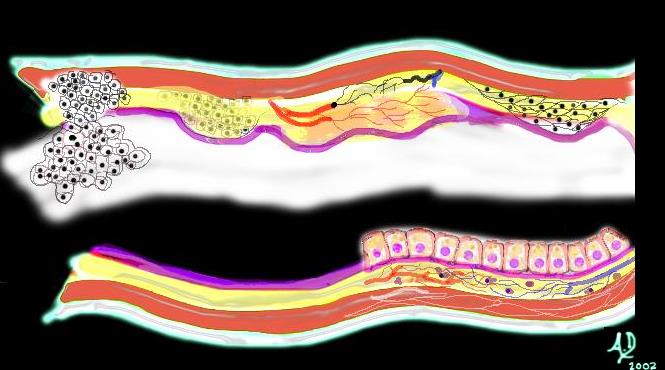
| The diagram shows a single columnar cell on the top side of the lumen that for whatever reason has been programmed to become “different” and instead of growing with characteristic columnar shape with pink nucleus and “peaches and cream” cytoplasm in this case has become round with white cytoplasm and black nucleus. It is a neoplasm – ie a new growth.
Courtesy Ashley Davidoff MD 32354 |
The single aberrant cell that develops at the initiation odf the diesease process, multiplies and forms its own community of cells that enlarges with time – and in its infancy is seen as a benign adenomatous polyp.
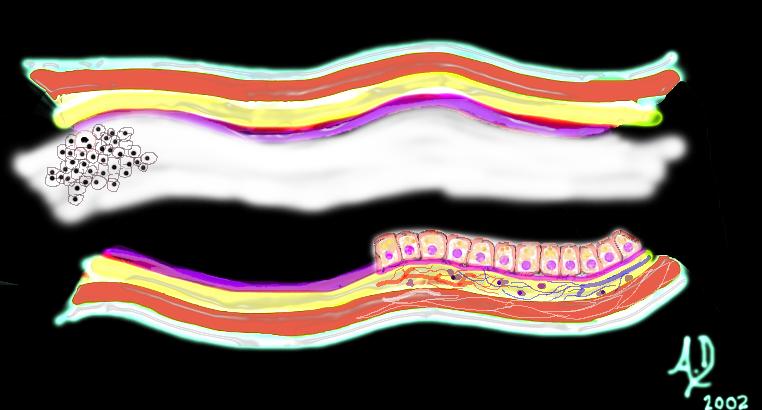 Mucosal disease -a benign polyp in its early stages Mucosal disease -a benign polyp in its early stages |
| Over time this neoplasm will continue to grow. If it grows slowly with monotony and uniformity in the morphology of cells, minding its own business and not disturbing its neighbors it is considered a benign neoplasm. It would be called a benign polyp and since it arises from the mucosa, it would be called an adenomatous polyp.
Courtesy Ashley Davidoff MD 32355 |
 5mm benign polyp 5mm benign polyp |
| This 5mm polyp is a common finding on colonic evaluation and at this size is a benign abnormality. Left intact it can grow into a monster. Hence it is usually removed by the endoscopist.
Courtesy Ashley Davidoff MD 12087 |
Most colonic polyps however (90%), are not adenomatous but are hyperplastic (size < 5 mm) meaning that they are still under the control of normal regulatory mechanisms of the body. Hyperplastic polyps are benign and, in most instances, are not considered premalignant. On the other 10% are adenomatous and are premalignant.
The endoscopist cannot distinguish between a hyperplastic polyp and a adenomatous polyp and therefore the endoscopist removes all polyps.
When polyps are less than a 1cms the possibility that they are malignant is less than 5%. As they grow into the 1-2cms range the chances of malignancy are in the 10% range. Once they grow beyond 2cms the chances of malignancy increase to 50%. There are three types of adenomatouis polyps; tubular, tubulovillous, and villous. Tubular adenomas are the most common while villous adenoma has the greatest potential to become malignant.
| Benign polyp – Virtual Colonoscopy |
| This series of images from a virtual colonoscopy shows an 8 mms polyp seen on the surface rendering images (salmon colored images) referenced to the sigmoid colon (bottom left) and with conventional CTimaging (bottom middle) At this size the polyp is almost certainly benign and can be removed through the colonoscope safely.
Courtesy Scott Tsai MD 45119 |
An adenomatous polyp if it is destined to become malignant usually takes 10-15 years to evolve. It will slowly invade the space of the lumen. but more importantly the space of the wall of the bowel, first into the submucosa and subsequently into the muscularis, serosa, adventitia lymphatics and finally into the systemic circulation.
 Malignant and aggressive growth Malignant and aggressive growth |
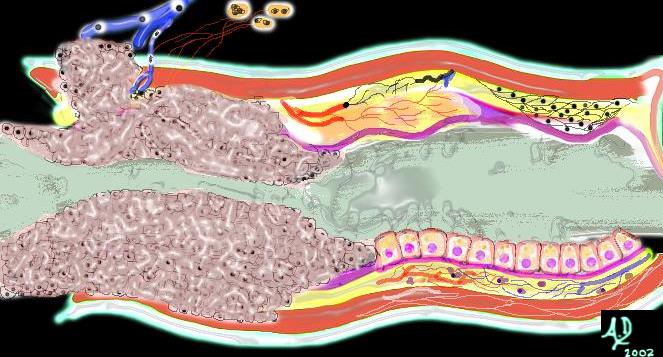
| The diagram illustrates the transformation from benign to malignant as the neoplasm starts to reveal an aggressive nature and invades and destroys surrounding tissue. In this instance it has advanced into the submucosa and muscularis as well as expanded into the lumen.
Courtesy Ashley Davidoff MD 32362b01 |
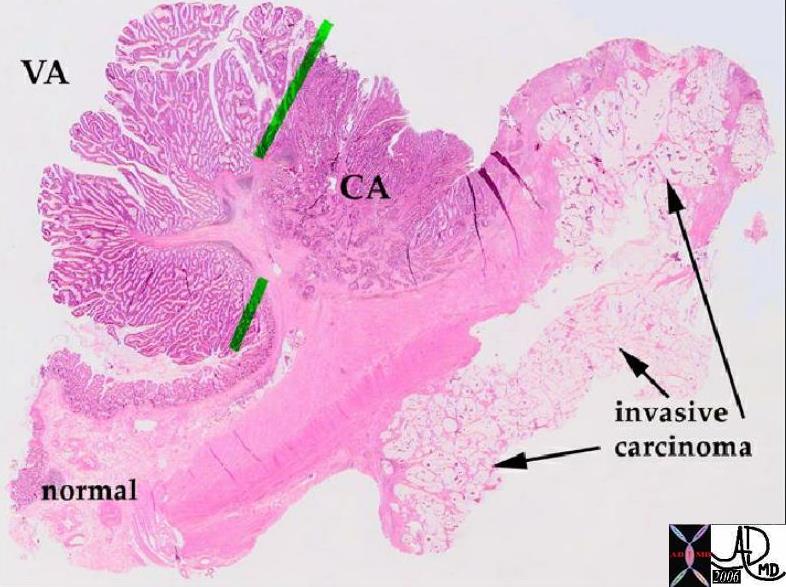 Pathology whole mount showing malignant transformation of a polyp Pathology whole mount showing malignant transformation of a polyp |
| In this pathology specimen the tree like morphology of the polyp is characterized by benign features to the left and superior with malignant features to the right and toward the base and below the green bars. The malignant disease extends into the deeper layers at the base.
Courtesy Barbara Banner MD 12160 |
 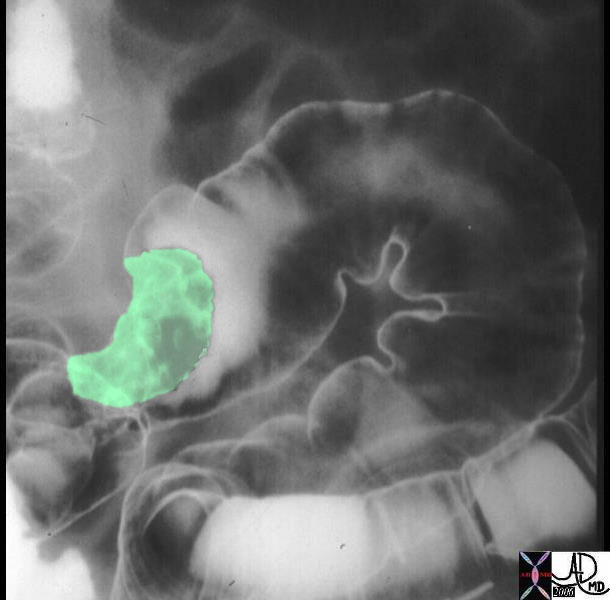 Irregular mass is seen in the sigmoid colon outlined by air and contrast of the double contrast enema. Irregular mass is seen in the sigmoid colon outlined by air and contrast of the double contrast enema. |
| The double contrast barium enema shows a large irregularly shaped mass in the sigmoid colon. The mass seen in green in the right sided image and is greater than 2cms in size, so that the risk of malignancy is substantially increased.
Courtesy Ashley Davidoff MD 12175 12175bo1 |

Ugly ulcerating malignant tumor |
| The grosspathology specimen shows an inflamed, angry looking mass in the colon that has central necrotic area surrounded by heaped tissue.
Courtesy Barbara Banner MD 02330 |
| Virtual colonoscopy showing an ulcerating cecal carcinoma |
| This series of images from a virtual colonoscopy shows a 5cms ulcerated mass seen on the surface rendering images (salmon colored images) referenced to the cecum (bottom left) and with conventional CT imaging (bottom middle) At this size and shape the mass is almost certainly malignant and cannot be removed through the colonoscope safely. Note how similar the morphology of this tumor is to the pathology of the specimen above (different patient)
Courtesy Scott Tsai MD 45123 |
As the disease progresses there is expansion of the tumor in the submucosa so that a circumferential lesion evolves. There may be extension into the deep layers of the wall, into lymphatics and portal venous system and eventually into the liver.
As the tumor grows locally it spreads circumferentially and eventually totally surrounds the bowel in a “napkin ring” like manner as depicted in the image below.
 Malignant growth through the all into veins and nodes Malignant growth through the all into veins and nodes |
| Left undiagnosed and untreated the malignant cells continue to grow without regard to the neighboring structures. It encircles the colon in “napkin-ring” fashion (as shown above) eventually blocking off the lumen and causing a bowel obstruction. It may grow through the wall and cause a bowel perforation and or grow into regional lymph nodes and portal venous radicles after which it will metastasize to the liver and other organs.
Courtesy Ashley Davidoff MD 32367b01 |
Radiologically the “napkin ring” translates into an apple core lesion when viewed radiologically and is best appreciated with a double contrast barium enema.
   Apple core lesion of the sigmoid colon Apple core lesion of the sigmoid colon |
| The double contrast barium enema shows an apple core lesion caused by circumferential growth of a malignant tumor of the colon in “napkin-ring” fashion. The second image shows the apple core-shape of the lumen. The third image shows the yellow mass of tumor that has surrounded the lumen in napkin ring fashion essentially strangling the lumen. Note how the distal colon which is receiving air and barium via the enema tip is relatively dilated when compared to the descending colon which is relatively decompressed suggesting an obstructive process. Note also the presence of contrast filled diverticuli at the rectosigmoid junction. The two entities of carcinoma and diverticulosis often coexist since diverticulosis is very common in Westernized nations.
Courtesy Ashley Davidoff MD 28655 |
 Napkin Ring Circunferential Tumor -aka Apple Core Napkin Ring Circunferential Tumor -aka Apple Core |
| Portion of left colon with a constricting carcinoma. The carcinoma has infiltrated the full thickness of the wall. This can be seen on the cut portion of the wall, where the wall is much paler than the surrounding mucosa.
colon large bowel fx apple core fx constriction fx narrowing fx wall thickening fx mass dx carcinoma malignant stricture grosspathology Courtesy Barbara Banner MD aka applecore12313 |
Cause and Predisposing Factors
Colon cancer is a disease that has its highest in developed countries such as the United States and Japan, and lowest in developing countries in Africa and Asia. It is interesting to note that in the US it has its highest incidence in African American men.
It is thought or appears to be closely linked to Western diet where high fat content and relatively low fiber content are considered major factors in the cause of the disease. In patients who develop colon cancer, it is thought that diet and other factors alter the genetics of a cell or a group of cells and an adenomatous polyp results. Most polyps will not evolve into cancer. A entity called multiple aberrant mutations seems to be the responsible process that will cause about 10% of adenomatous polyps to evolve into cancer. This process disinhibits normal regenerative processes, and enables the mucosa to advance from an adenomatous polyp into a carcinoma over 10-15years. Evolving work on the genetic aberrancies is allowing advances in both the diagnosis and treatment of the disease. Identifying the genetic mutation of a cell in the stool may prove to be an important screening technique. Another example is the DCC gene, which causes the neoplastic cells to adhere to each other. The absence of this gene in the mutated gene would decrease cell adherence and theoretically enable malignant cells to metastasise easily. Thus testing for the DCC gene may shed light on the virulence and natural history of colon carcinoma in a particular patient and thus aid in prognostication.
Other known associated diseases include a prior history of colon carcinoma (metachronous = multiple separate occurrences – 4-5% of colon cancers), synchronous lesions (two or more at the same time = 1%) and inflammatory bowel diseases (IBD). Ulcerative colitis is a well esatablished associated disease, while the association with Crohn’s colitis is less common.
 Synchronous Tumors Lying Side By Side in the Cecum Synchronous Tumors Lying Side By Side in the Cecum |
| Two tumors lie side by side in the cecum. The polyp on the left was a large villous adenoma with malignant potential and the lesion on the right was a carcinoma.
12070 colon large bowel cecum ileocecal valve fx mass masses dx villous adenoma dx carcinoma malignant primary tumor cancer grosspathology Courtesy Barbara Banner MD |
Hereditary factors that predispose to colon cancer are seen in conditions such as familial polyposis and Gardener’s syndrome, where there is a very strong association. (see below) Other conditions such as prior history of breast or endometrial carcinoma and retinitis pigmentosa also raise the awareness of associated colonic carcinoma.
Familial Adenomatous Polyposis
Familial adenomatous polyposis (FAP) is the most common adenomatous polyposis syndrome, and it is characterized by the presence of innumerable neoplastictubular adenomatous polyps of the colon. The cause of the disease relates to an autosomal dominant inherited disorder. In early life (about 16 years) the genetic defect evolves into and results in a colonic mucosa that is carpeted with hundreds to thousands of adenomatous polyps. In 100% of patients the syndrome is complicated by the development of cancer at the age of 30 – 40years, and hence all patients should be treated with colectomy in early years of the disease. (teenage to early 20’s)
Associated diseases include desmoid tumors (4-30%) and other rarer associations including medulloblastoma, thyroid cancer, adrenal cancer, gastric cancer and pancreatic cancer.
The diagnosis is established in patients who have a positive family history and by colonoscopy demonstrate more than 100 polyps.
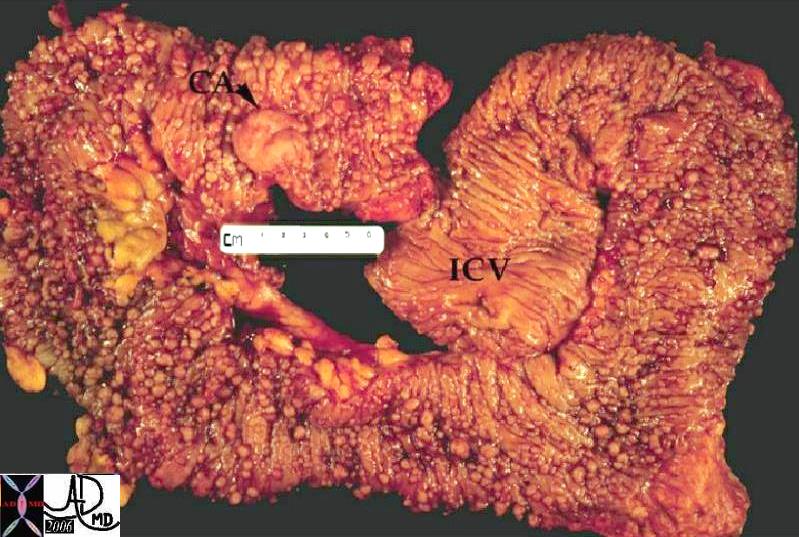 Familial Polyposis Syndrome with Carcinoma Familial Polyposis Syndrome with Carcinoma |
| The normal mucosa in this patient has been replaced by inumerable carpet of polyps extending throughout the colon. A malignancy has evolved (“ca” = carcinoma) at the distal end of the colon. |
Clinically it is usually asymptomatic and only presents presents once the patient has developed cancer. Symptoms include abdominal pain, diarrhea, mucus diarrhea, and bloody diarrhea.
Colonoscopy is the imaging and diagnostic study of choice since the diagnosis can be established and biopsy of suspicious lesions can be accomplished.
Colectomy with mucosal proctectomy and ileoanal pouch pull-through is the therapeutic procedure of choice
References
eMedicine Familial Adenomatous Polyposis
Gardner’s Syndrome
Gardners syndrome is an autosomal dominant inherited disease of the soft tissues, and is a variant of familial adenomatous polyposis syndrome. It is characterized by multiple osteomas, gastrointestinal polyps, and skin and soft tissue tumors. Cutaneous findings include epidermoid cysts, and desmoid tumors. The resulting osteomas are characteristic of the disease and their presence is a prerequisite to the diagnosis. They most commonly occur in the mandible but also in the skull. The colonic polyps appear in puberty and have a 100% risk of progressing to malignant disease between 30 and 40 years. The diagnosis is suspected clinically if there is a family history of the disease, or a young patient presents with multiple cutaneous lesions that may include epidermoid cysts, or other unusual skin lesions such as lipomas fibromas or neurofibromas at a young age. Imaging includes a skull X-ray to evaluate for osteomas and colonoscopy is indicated as well particularly if osteomas are present. Polyps usually are seen only once the osteomas are present.
Treatment options depend on the findings at colonoscopy. If more than 30 polyps are found, colectomy and stripping of the rectal mucosa is recommended because of the high risk of rectal carcinoma.
Thereafter there should be a continued surveillance for other associated tumors including hepatoblastoma, skeletal tumors, brain tumors and thyroid carcinoma.
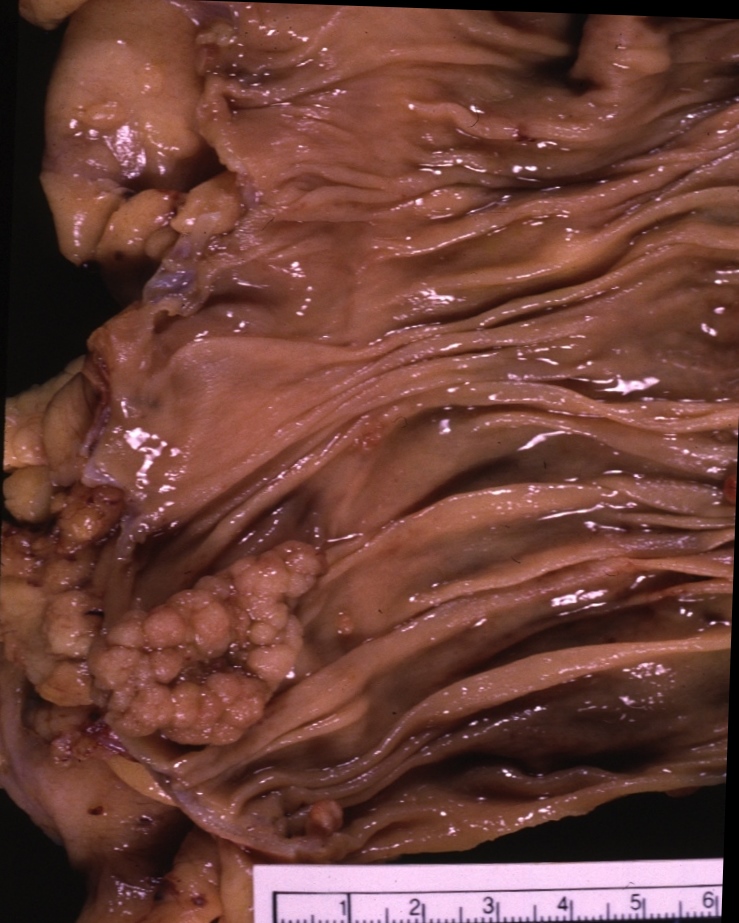
 Gardner’s Syndrome – Polyps and Carcinoma Gardner’s Syndrome – Polyps and Carcinoma |
| 12182 colon large bowel rectum fx mass fx multiple polyps dx Gardner’s syndrome complicated by rectal carcinoma Gardners syndrome grosspathology Courtesy Barbara Banner MD 5star |
References
Gardner, EJ: A genetic and clinical study of intestinal polyposis, a predisposing factor for carcinoma of the colon and rectum. Am J Hum Genet 3: 167-176, 1951.
Ulcerative Colitis
Ulcerative colitis is an idiopathic inflammatory process of the mucosa of the colon and rectum, and is characterized by its involvement of the the rectum, and retrograde progressive involvement of sigmoid then descending, transverse and ascending colon. It is in essence a mucosal disease. The cause of the disease is unknown but the result is mucosal inflammation and ulceration. The risk of cancer increases with the chronicity and extent of the disease. About 5% of patients with UC develop colon cancer. As chronicity increases and extent of involvement increases the incidence of colon cancer also increases. Carcinoma is usually preceded by a dysplastic phase. Patients who have had a pancolitis for 8 years should receive a screening colonoscopy and biopsy, while those whose disease is restricted to the left colon should have screening colonoscopy and biopsy after about 12 years from the onset of disease. The biopsy is taken every 10cms at a random location. All patients with IBD should have repeat colonoscopy and biopsy every 2-3 years. These recommendations have been endorsed by the American Cancer Society, the American College of Gastroenterology, the American Society of Colon and Rectal Surgeons, and the Crohn’s & Colitis Foundation of America.
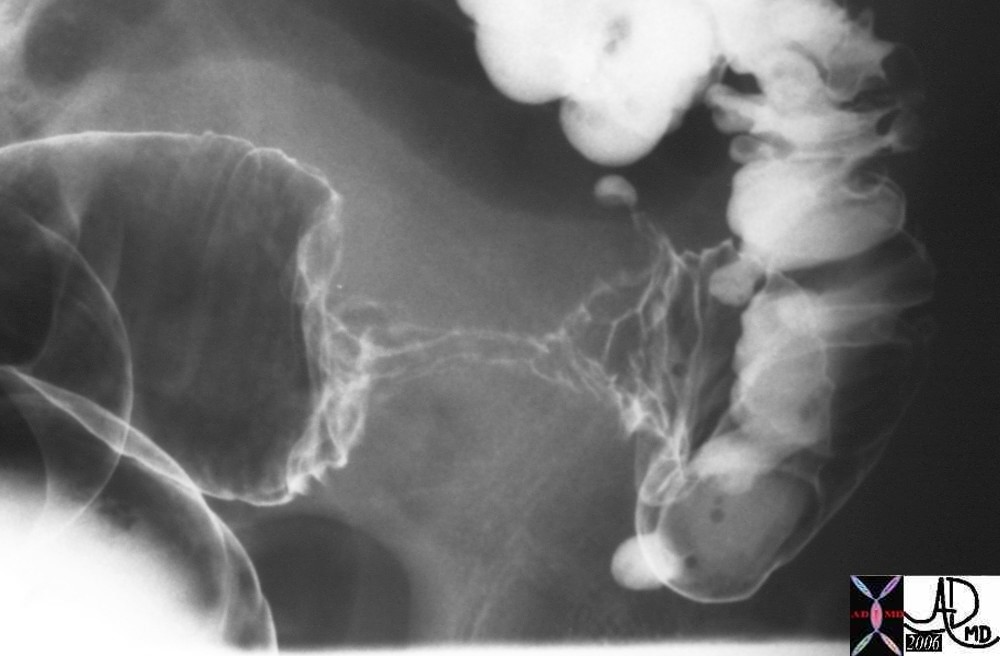
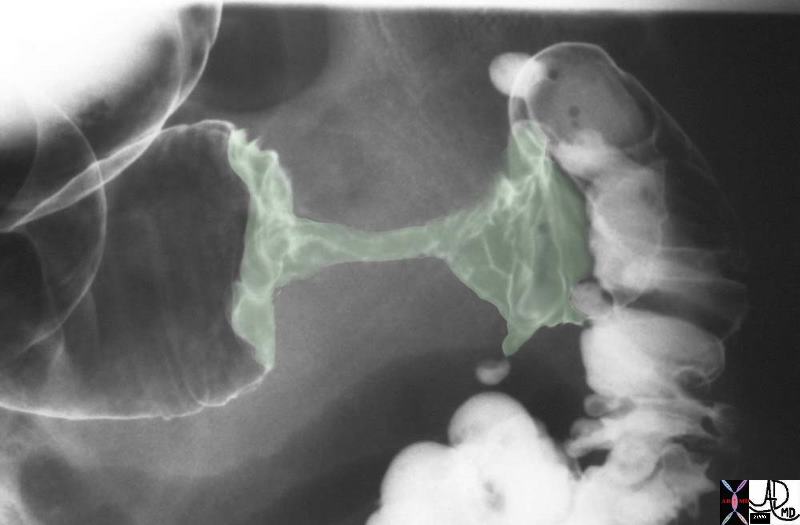
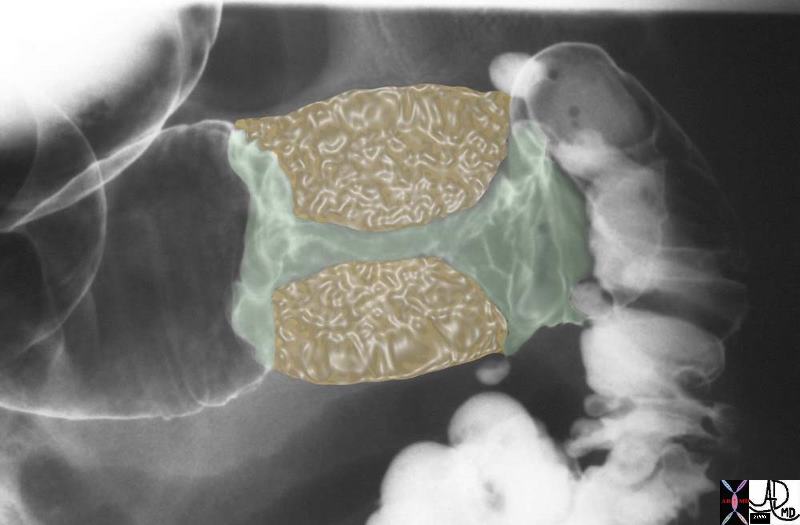
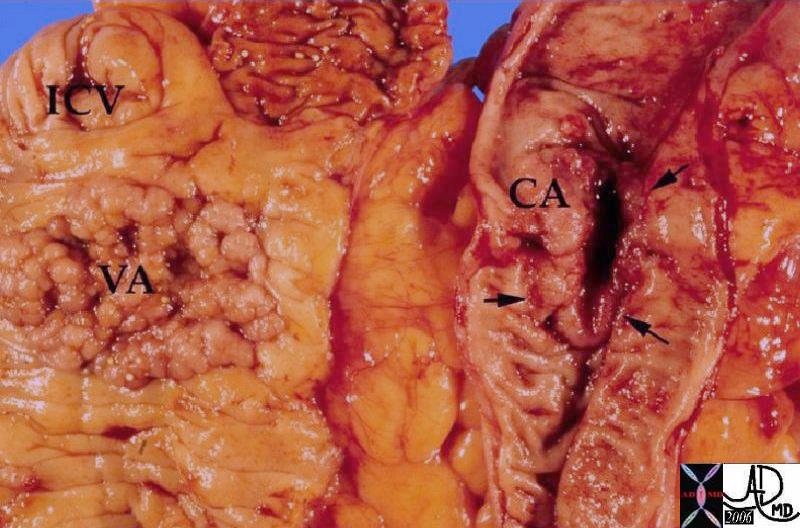
 Colon Carcinoma in a Background of Chronic Ulcerative Colitis Colon Carcinoma in a Background of Chronic Ulcerative Colitis |
| This is a resected right colon open longitudinally in a patient with chronic ulcerative colitis. This patient had two simultaneous carcinomas. In this picture the terminal ileum and the ileocecal valve and a protruding appendix are present to the right of the label. Just beyond this, in the ascending colon, there is a thickened, strictured area which represents one of the carcinomas. Notice how ill defined and poorly seen this tumor is. The carcinomas in ulcerative colitis tend to be very difficult to see grossly. Beyond this first carcinoma the bowel mucosa is irregularly flattened indicating an old area of regenerated ulcer. At the opposite end of the specimen is another thickened strictured area which represents the second carcinoma.
colon large bowel fx masses fx ulcerating dx UC ulcerative colitis dx carcinoma malignant 12864 Ulcerative Colitis: carcinoma. transformation cancer grosspathology Courtesy Barbara Banner MD
|
Statistics
Adenocarcinomas of the colon are the most common cancers seen in the GI tract in western society. 1 in 20 Americans will develop colon cancer and 150,000 new diagnoses will be made each year and about 50,000 patients will die of the disease per year. While it ranks third among both men and women in mortality in western society, it is really second to lung cancer in women and second to lung cancer in men because men do not get breast cancer and women do not get prostate cancer.
Both men and women face a lifetime risk of nearly 6% for the development of invasive colorectal cancer. The disease is most common after the age of 70, but in the patient at high risk such as those with familial syndromes, colonic carcinoma could present in the late twenties or 30’s , while in the general population it could occur as early as the 40’s.
Pathology
Most tumors are adenocarcinomas. The most common site is the sigmoid colon (20%) followed by rectum (15%), transverse colon (12%), descending colon (10%), ascending colon (8%) and cecum (8%). As the population ages there is a tendency for the right sided colonic carcinomas to become more common. In ulcerative colitis, since the longest standing inflammation is left sided it is not surprising that left sided colon carcinoma is more common.
 This polyp is greater than 2cms and was malignant on histopathologyical examination This polyp is greater than 2cms and was malignant on histopathologyical examination |
| The distinction between a malignant polyp and a benign polyp is sometimes difficult to discern based on gross pathology, but as the lesion becomes greater than 2cms., concern for malignant change should be considered. In the above specimen, there were no signs of overt malignancy other than its size, and the histopathology showed malignant change.
00317 colon cecum fx mass dx carcinoma dx cancer grosspathology Courtesy Ashley Davidoff MD |
| Ulcerating Colon Carcinoma |
| This specimen has obvious malignant characteristics macroscopically, characterized by heaped edges and central ulceration.
Note 02499 colon large bowel fx mass fx ulcerating mass fx raised edges fx central necrosis dx carcinoma malignant primary tumor cancer grosspathology Courtesy Dr Gutkin MD |
 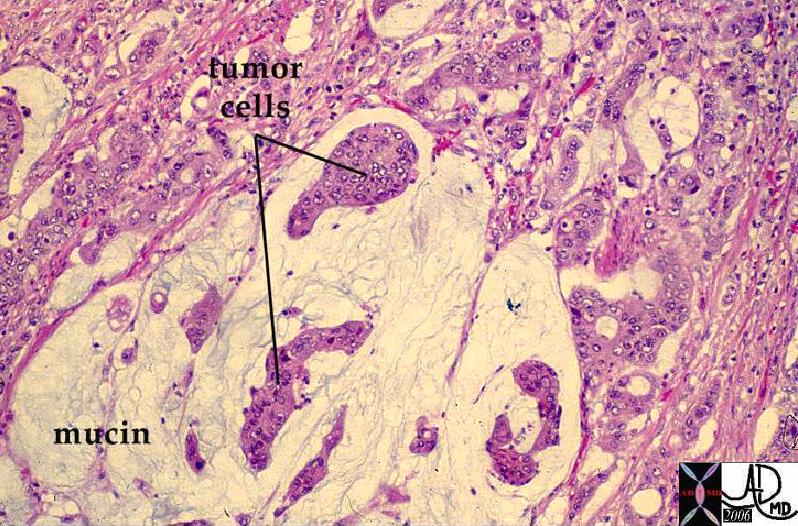 Normal Colonic Mucosa (left) and Mucin Secreting Colon Carcinoma (right) Normal Colonic Mucosa (left) and Mucin Secreting Colon Carcinoma (right) |
| The image on the left shows the normal crypts while the image on the right shows a mucin secreting adenocarcinoma. The most obvious difference between the two images is the nuclear cytoplasmic ratio. Note in the case on the right, the cancer nuclii are large and heterogeneous while there is a relative paucity cytoplasm.
12860 12208 colon large bowel fx mucin secreting fx mucinous accumulation dx carcinoma mucin secreting adenocarcinoma histopathology Courtesy Barbara Banner MD ask
|
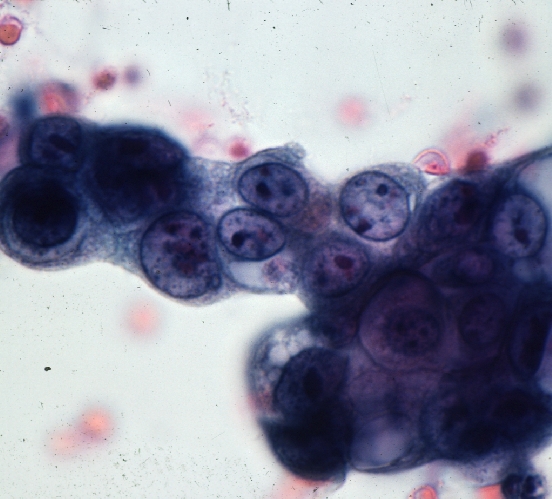 Colon Carcinoma – Cytopathology Colon Carcinoma – Cytopathology |
| These cells represent a group of malignant cells characterized by large heterogeneous nuclii and a paucity of cytoplasm. The nuclear to cytoplasmic ratio is high and this feature is characteristic of malignant cells.
44834 colon large bowel dx carcinoma mucin mucinous histopathology cytopathology Courtesy Barbara Banner MD ask |
Potential Complications
The most common site for metastases is the liver (25%), mesenteric and retroperitoneal nodes (15%), kidney obstruction (10%). Large bowel obstruction, perforation and intussusception are potential complications of the disease.
Hematogenous Spread – Liver Metatsases
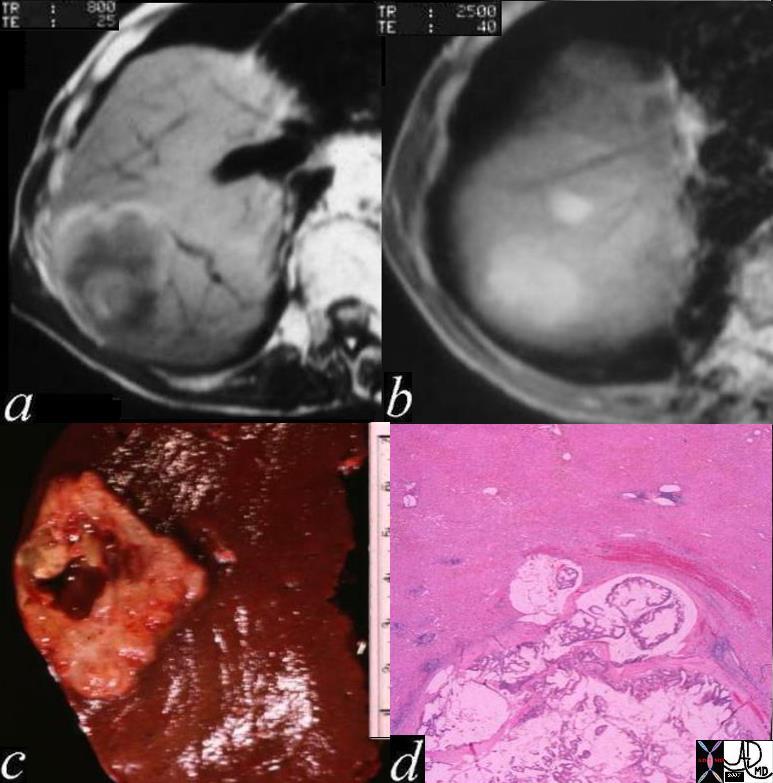 Carcinoma of the Colon with Metatstasis to the Liver Carcinoma of the Colon with Metatstasis to the Liver |
| The MRI of the liver shows a space occupying abnormality at the dome of the liver with central hyperintensity on T1 weighted image, (a) as well as diffuse hyperintensity on T2 weighting (b) representing a hemorrhagic mucin secreting adenocarcinoma seen on the gross specimen (c) and on the histological; section (d).
03028c02 liver hepatic mass a = T1 weighted central intensity rim and matrix of low intensity periphery b = T2 weighting = T2 bright c = gross pathology hemorrhagic lesion d = mucin secreting metastasis with hemorrhagic ring fx metastattic colon carcinoma mucin secreting adenocarcinoma with central hemorrhage peripheral hemorrhage MRIscan histopathology grosspathology Davidoff MD |
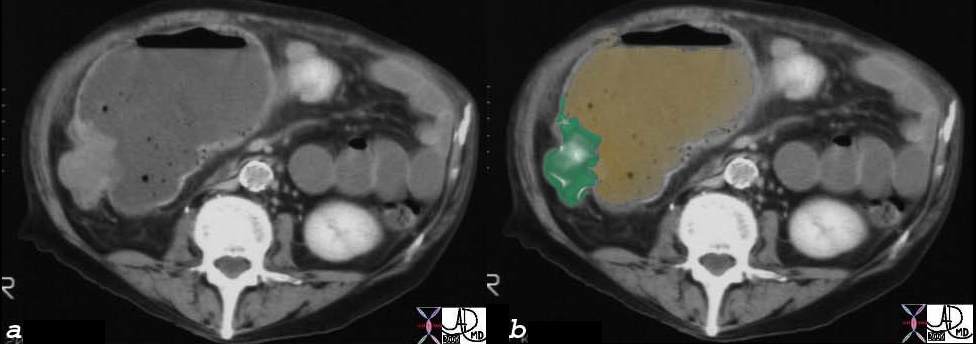
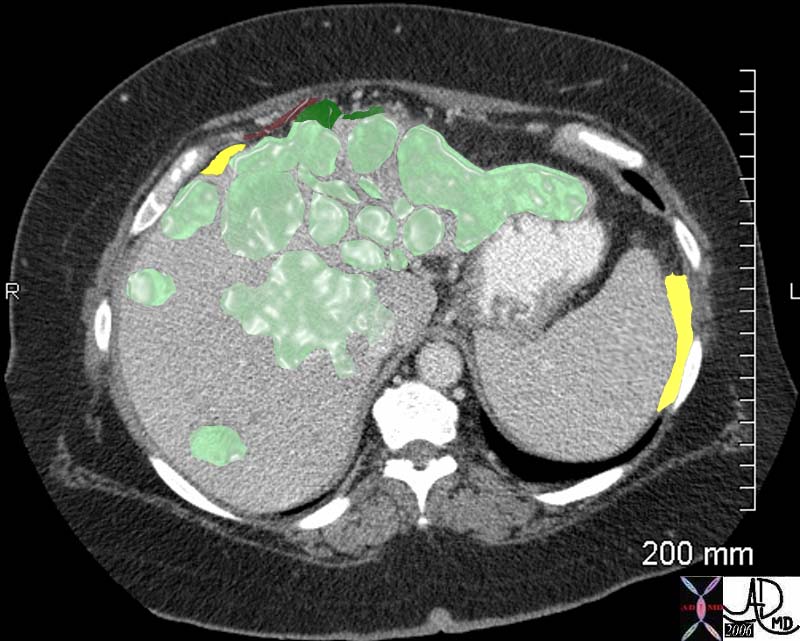 Colon Carcinoma with Multiple Metastases to the Liver and Involvement of the Capsule Colon Carcinoma with Multiple Metastases to the Liver and Involvement of the Capsule |
| The abdominal CT is from a middle aged female with right sided discomfort. The image reveals multiple space occupying lesions (light green) in the liver. The patient was found to have a primary colonic carcinoma. The capsule of the liver is involved by tumor extending to the surface of the liver and deforming the surface (dark green). The disease is also close to the diaphragm (maroon). The involvement of the liver capsule and possibly the right hemidiaphragm is likely the cause of the patients pain. There is also a small amount of ascites present (yellow) either as a response to involvement of the liver capsule or the early development of malignant ascites.
45051 45051b04 middle aged female with right sided discomfort liver diaphragm fx enlarged hepatic enlargement hepatomegaly fx hepatic masses shrunken left lobe fx abdominal ascites dx colonic carcinoma with hepatic metastasis (metastatic liver disease) metastases with diaphragmatic and renal displacement from the large liver ascites probably malignant note hepatic capsule is involved abdominal CTscan of the abdomen Courtesy Ashley Davidoff MD 45049 45050 45051 45052 45053 45054 |
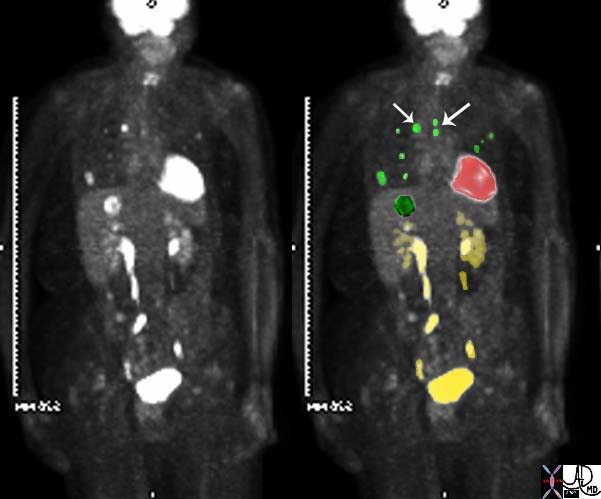 Sigmoid Carcinoma with Metastases to the Liver and Lung (green) Sigmoid Carcinoma with Metastases to the Liver and Lung (green) |
| The PET scan in this elderly female with known carcinoma of the sigmoid colon shows metastatic disease to the liver, (dark green), lungs (light green) and mediastinum (light green with arrows) There is normal increased acivity in the heart (red) and excretion of the FDG into minimally dilated collecting systems (yellow).
45132c03 elderly female with known sigmoid colon carcinoma liver lungs mediastinum fx FDG positive uptake fx high intensity uptake in a single focus in the dome of the right lobe of the hepatic parenchyma meadiastinal lymph nodes and within the pulmonary parenchyma dx colonic mucinous adenocarcinoma complicated by metastatic lung disease and hepatic metastasis PETscan Courtesy Ashley Davidoff MD 45132 45133 45134 45135 45136 45139 45141 |
Lymph Node Metastases
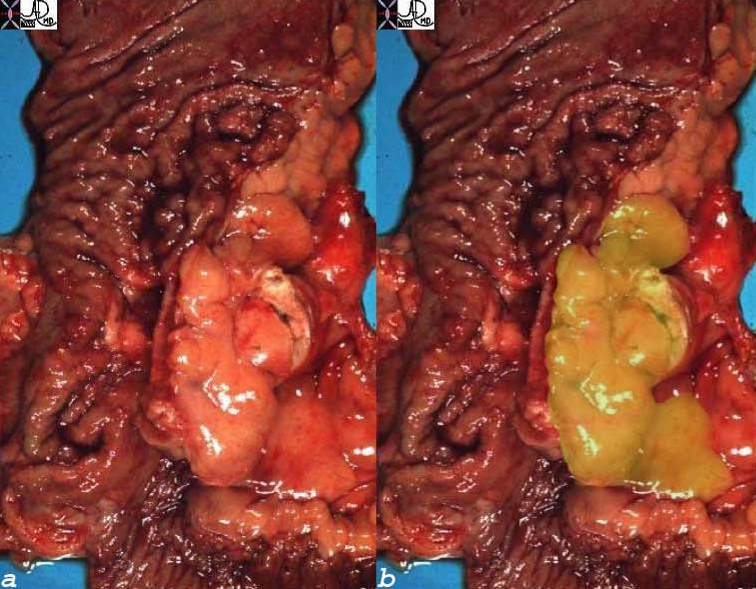 Regional Lymph Node Enlarged Regional Lymph Node Enlarged |
| The pathology speimens are from a patient with long standing ulcerative colitis complicated by carcinoma. The nodule (overlaid in orange represents an enlarged regional lymph node that was positive for malignancy.
12196c01 colon large bowel lymph node dx enlarged fx invaded dx colonic carcinoma with metastasis lymphadenopathy grosspathologyu Courtesy Barbara Banner MD |

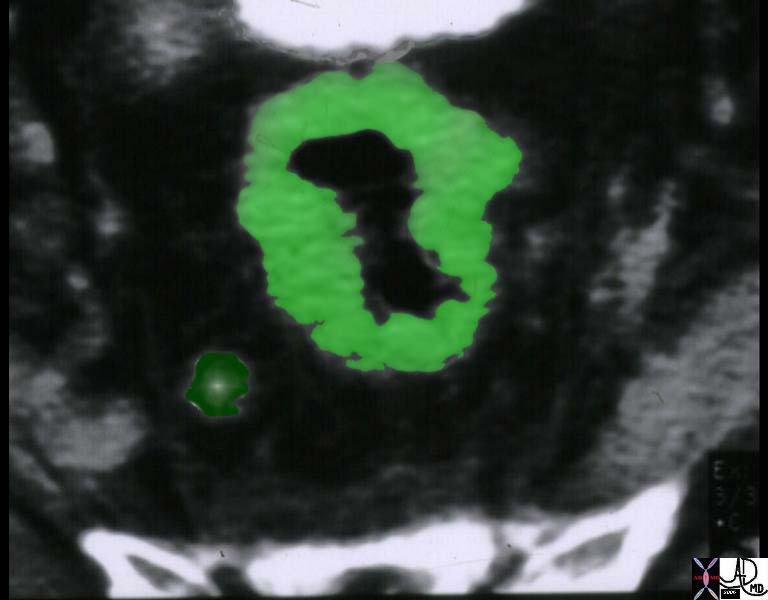 Rectal Carcinoma with a Perirectal Node Rectal Carcinoma with a Perirectal Node |
| The CT scan of the rectosigmoid region shows diffuse thickening of the rectum (light green) with an abnormal lymph node in the perirectal fat (dark green) in this patient with carcinoma.
colon large bowel rectum fx rectal wall thickening fx nodule lymph node dx rectal carcinoma primary malignant tumor cancer CTscan Courtesy Ashley Davidoff MD 12092 12092b01 |
Local Extension
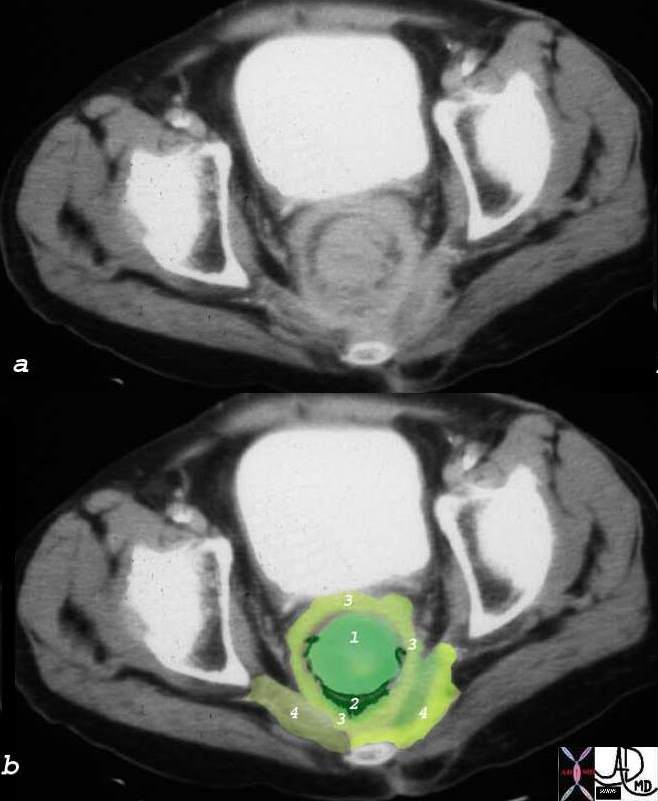 Obsructing Rectal Carcinoma with Extension into Levator Ani and Pelvic Wall Obsructing Rectal Carcinoma with Extension into Levator Ani and Pelvic Wall |
| CT scan through the rectum shows a large mass (1) extending through the perirectal fat (2) and into the levator ani (3) and progressing into the lateral pelvic wall (4)
00885c03 colon large bowel rectum mass carcinoma extension to levator ani pelvic sidewall CTscan Courtesy Ashley Davidoff MD |
Bowel Obstruction
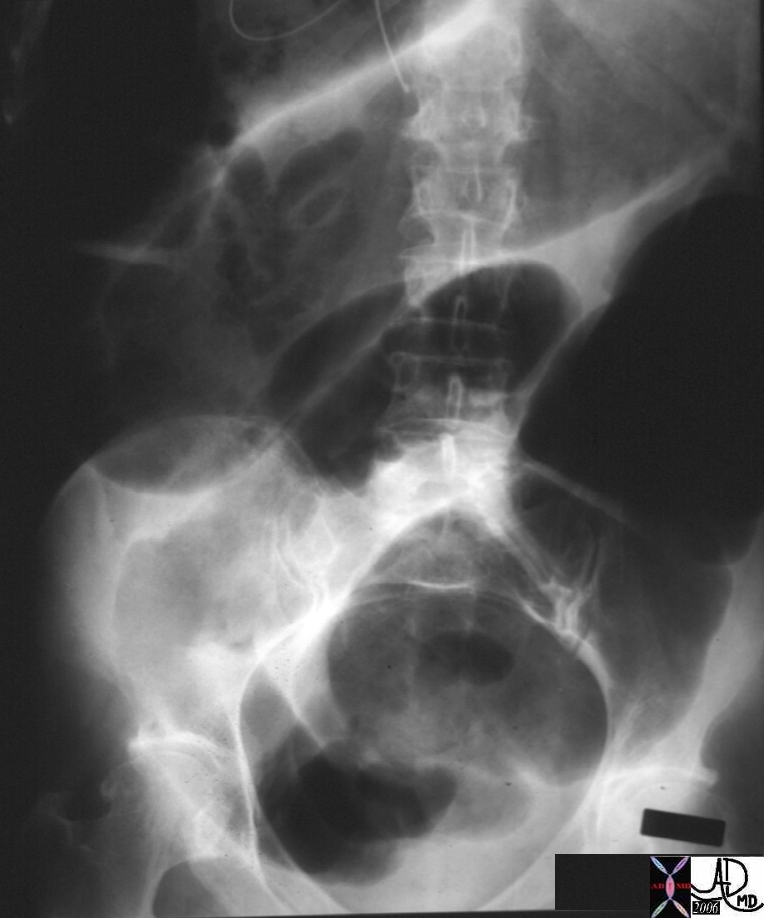 Colonic Distension No Rectal Air Colonic Distension No Rectal Air
The Diagnosis was Large Bowel Obstruction Secondary to a Rectal Tumor |
| 00879 hx 55M with distension abdomen colon large bowel rectum fx enlarged dilated dx rectal carcinoma malignant tumor dx large bowel obstruction LBO KUB abdominal plain film Courtesy Ashley Davidoff MD |
 Obstructing Colon Carcinoma with Upstream Dilatation Obstructing Colon Carcinoma with Upstream Dilatation |
| 28683c01 colon obstruction LBO large bowel obstruction colon carcinoma dilated obstructed CTscan Courtesy Ashley Davidoff MD |
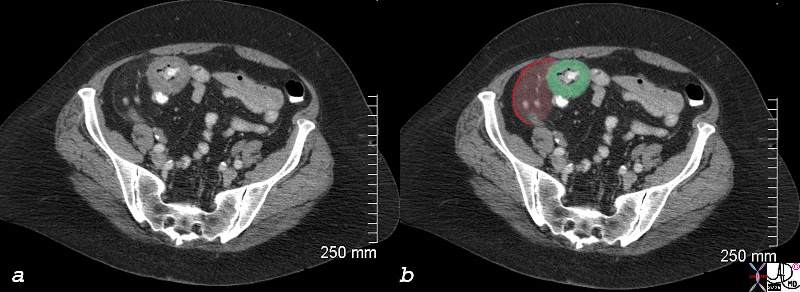 Cecal Carcinoma with Peritoneal Involvement presents with RLQ Pain Cecal Carcinoma with Peritoneal Involvement presents with RLQ Pain |
| 83037c03.8s 70 F presents with right lower quadrant pain RLQ colon cecum mass colon carcinoma napkin ring peritoneum peritonism somatic pain induration CTscan Courtesy Ashley Davidoff MD copyright 2008 |
Diagnosis
In general colon carcinoma is symptomatically occult and patients in general are asymptomatic in the early stages but may present with anemia and hemoccult positivity. As the anemia progresses the patients may present with weakness and weight loss and occasionally with abdominal pain
The diagnosis of colon carcinoma as the 2nd most common cause of death from malignancy in the US should be on the mind of caregivers in all patients starting at about the age of forty where unexplained hemoccult positive test or occult anemia should be viewed with high suspicion. Such a patient should undergo colonoscopy as the diagnostic study of choice. All patients should be screened with colonoscopy after the age of 50 years and thereafter every 10 years.
In addition to the colonoscopy annual fecal occult blood testing (FOBT) and periodic flexible sigmoidoscopy. Alternatively barium enema should be used every 3-5 years. (Helm)
Despite the guidelines a large prportion of the US population are not being screened because of insufficient numbers of trained colonoscopists to meet the need, fear of the procedure, or ignorance of the guidelines. CT colonography is an excellent alternative for screening when colonoscopy is not possible. Sensisitivity for small polyps is high and is similar to that of optical colonoscopy.
Lab Tests
In the patient with suspected colon carcinoma, blood tests should include cell count and hematocrit for the evaluation of anemia. The serum carcinoembryonic antigen (CEA ) is a tumor marker most often used for the evaluation of gastrointestinal tract malignancies. In about 60% of patients with colon carcinoma it is elevated and it is therefore a worthwhile test to obtain. It is also reasonable to evaluate liver function tests in the patient with suspected colon carcinoma to evaluate for the presence of liver metastases, though a negative result does not exclude the diagnosis.
Imaging
Optical colonoscopy is the study of choice for the patient with suspected carcinoma since it offers the opportunity to biopsy suspicious lesions, and to remove small polyps. When this method fails or is not possible, then CT colonography has now become the second line diagnostic study of choice. Fly through cecal carcinoma
Once the diagnosis is established a CTscan of the abdomen is used for staging the disease preoperatively. The local disease and extension into pericolic fat and lymph nodes can sometimes be established. Liver involvement is also best evaluated at this time with and if necessary suspicious lesions can be biopsied or further chharacterized with MRI.
It is also reasonable to perform a chest X-ray preoperatively to aid in staging though sensitivity for small lesions is low.
Treatment and Management
Surgery
A right, transverse or left hemicolectomy encompassing the lymphdrainage area is standard surgical care. At the time additional staging procedures are critical in the management. regiomnal lymph nnodes should be removed for pathological evaluation, nodular lesions in the peritoneal cavity should also be evaluated, and the liver should be exanmined with ultrasound and suspicious lesions biopsied as well.
Thereafter it is important to stage the disease when all the data is gathered to assess the post operative management
Staging
Two classifications have been of use: the TNM ([primary] tumor, [regional lymph] node, [remote] metastasis) staging and the Dukes classification.
TNM Staging System for Colon Cancer
| Stage | Primary Tumor (T) | Regional Lymph Node (N) | Remote Metastasis (M) |
|---|---|---|---|
| Stage 0 | Carcinoma in situ | N0 | M0 |
| Stage I | Tumor may invade submucosa (T1) or muscularis (T2). | N0 | M0 |
| Stage II | Tumor invades muscularis (T3) or perirectal tissues (T4). | N0 | M0 |
| Stage IIIA | T1-4 | N1 | M0 |
| Stage IIIB | T1-4 | N2 | M0 |
| Stage IV | T1-4 | N2 | M1 |
*N0: No regional lymph node metastasis.
N1: Metastasis in 1 to 3 regional lymph nodes.
N2: Metastasis in 4 or more regional lymph nodes.
Dukes Classification
| Stage | Characteristics |
|---|---|
| Dukes stage A | Carcinoma in situ limited to mucosa or submucosa (T1, N0, M0) |
| Dukes stage B | Cancer that extends into the muscularis (B1), into or through the serosa (B2) |
| Dukes stage C | Cancer that extends to regional lymph nodes (T1-4, N1, M0) |
| Dukes stage D | Modified classification; cancer that has metastasized to distant sites (T1-4, N1-3, M1) |

Endoscopic Ultrasound Showing a 1.5cms Rectal Tumor That Has Extended into the Submucosa and Muscularis In the TNM classification sytem it would be a T3 lesion |
| 00896 colon rectal rectum fx mass dx colon carcinoma endoscopic USscan Courtesy Ashley Davidoff MD |
Treatment
Stage 1 and 2 cancers are treated with surgery alone and have a very high cure rate. Stage 1 disease has a 90 to 95 percent five-year survival and early stage 2 disease (B-1) has an 85 percent five-year survival. Once the tumor invades the muscularis layer (advanced stage 2 or B-2, T3N0M0) treatment protocols are more controversial as to whether post operative chemotherapy offers advantage. The overall five-year survival with surgery alone in this group is 70 percent.
Stage 3 disease (node positive)benefits from postoperative chemotherapy. The overall five-year survival in this stageranges from 25 percent to 60 percent.
Stage 4 metastatic colon cancer occurs in approximately 30% of all patients diagnosed with the disease. If metatstatic disease is not identified within 5 years of diagnosis it would be quite unusual for it to develop at all. Patients with isolated liver metastases may benefit from resection, and if surgery is contraindicated then alternative techniques such as cryoablation radiofrequency ablation or stereotactic radiation. Systemic chemotherapy is an option for patients who cannot undergo the above options and a combination chemotherapy may cause regression in 20-25% of patients. The average survival for patients with metastatic colon cancer is between 12 and 18 months, and 5 year survival is approximately 5%.
Conclusion
Colon carcinoma is a common disease, and its pathogenesis from an adenomatous polyp to a malignancy is between 10-15 years. The colon offers a unique window for the endoscopist or radiologist by exposing its entire mucosa to the examining scope, and thus small early lesions can be visualized, biopsied and treated. Hence if all patients and their caregivers would adhere to screening protocols for both the common and uncommon forms, early detection and hence treatment and cure can be accomplished. The challenge is to create a system where screening techniques are made available to all.
References
American Cancer Society. Cancer facts & figures–2001. Atlanta, Ga.: American Cancer Society, 2001. Retrieved September 2001 from: www.cancer.org.
Helm JF, Sandler RS. Colorectal cancer screening. Med Clin North Am 1999;83(6):1403-1422, vi.
Ries LA, Miller BA, Hankey BF, eds. U.S. Dept of Health and Human Services, Public Health Service. SEER cancer statistics review, 1973-1991: tables and graphs. Bethesda, Md.: National Institutes of Health, 1994; NIH publication no. 94-2789:151.
Morson BC. The evolution of colorectal carcinoma. Clin Radiol 1984;35:425-31.
Rozen P. The OMED Colorectal Cancer Screening Committee: a report of its aims and activities. Organisation Mondiale d’Endoscopie Digestive. Gastrointest Endosc 1999;50:453-4.
Byers T, Levin B, Rothenberger D, Dodd GD, Smith RA. American Cancer Society guidelines for screening and surveillance for early detection of colorectal polyps and cancer: update 1997. American Cancer Society Detection and Treatment Advisory Group on Colorectal Cancer. CA Cancer J Clin 1997;47:154-60.
Web References
MCQ
The
Colon carcinoma is a malignant condition of the colon with the causes being multifactorial but resulting in a mass or a narrowing in the large bowel.
UNDER CONSTRUCTION
UHRad Case report