| Blood Supply of the Colon
The Common Vein Coyright 2007 IntroductionThe superior mesenteric artery (SMA), inferior mesenteric artery (IMA), and internal iliac arteries are the vessels that supply the colon. The SMA is the artery of the midgut while the IMA is the artery of the hindgut. The distal and terminal portion of the hindgut is supplied by the rectal branches of the internal iliac arteries.
SMAThe SMA, as the midgut artery supplies the right side of the colon from the ileocecal valve to the region of the distal transverse colon and splenic flexure. The SMA shares the supply of the splenic flexure with the IMA, and therefore does theoretically help supply the proximal hindgut. The SMA arises from the aorta between T12 and L2. The usual branches of the SMA to colon include the ileocolic artery, the right colic artery and the middle colic artery, supplying in general the cecum ascending colon and transverse colon respectively. The ileocolic artery almost always arises directly from the SMA. The right colic may arise from the SMA, but sometimes arises from one of its branches – the ileocolic or the middle colic artery. The middle colic artery strangely arises from the SMA from a more proximal position in the SMA than the ileocolic even though it supplies colon that is more distal in location. Its origin is at the first part of the SMA close to the origins of the jejunal branches. The branches course in the mesentery and extend to the medial and mesenteric edge of the ascending colon, and then branch so that they course and connect along the inner margin of the colon forming the marginal artery allowing the branches to connect with each other. In the transverse colon the mesenteric edge is posterior and hence the marginal artery is posterior. The vasa recta (recta = straight) branch from the marginal artery and course over the colon finally penetrating the wall of the colon to form a capillary network in the submucosa. Once the vessels proceed beyond the marginal artery and into the bowel wall, there are not usually collateral pathways so that any occlusion beyond the marginal artery will result in ischemia.
The SMA and celiac axis connect through the pancreaticoduodenal arcade that runs through the head of the pancreas and also connect to some extent through the transverse pancreatic artery that runs through the body and tail of the pancreas. The arc of Buehler is an embryologic connection between the SMA and celiac axis that is seen uncommonly as a persistent communication. The SMA also connects to the IMA via the marginal artery on the left side of the colon. Thus the three major arteries and circulations do have important connections that become life saving when one becomes narrowed or blocked.
Applied AnatomyDisorders of the SMA arterial circulation are relatively common including bowel ischemia from thrombosis, embolization, dissection, and hypotension. Disorders that lead to lower GI bleeding include angiodysplasia and diverticular disease. The following case is from a 71 year old male who presented with brisk rectal bleeding and hemodynamic instability.
IMAThe IMA originates from the aorta around L3 and is a fairly small vessel arising at an acute angle. One therefore has to choose a catheter that has an acute angle in order to engage this vessel for selective catheterization. In its proximal portion the vessels parallels the aorta for about 3-4cms. Its branches include the left colic, sigmoid branches and superior rectal artery. As stated above it connects with the SMA via the marginal artery with a watershed region created in the splenic flexure. Since this region is an end arterial circulation for the SMA and IMA it is potentially a weak link in the circulation predisposing it to ischemia. There are three major branches of the IMA including the left colic artery, sigmoid arteries (usually about 2-3 vessels) and the superior rectal artery (aka superior hemorrhoidal artery).
Internal iliac arteriesThe iliac supply includes mid to distal rectum and anal regions. They provide an important collateral pathway between the systemic circulation at large with the mesenteric circulation. The middle and inferior rectal branches supply the distal rectum and anal regions.
The single superior rectal artery arises from the terminal portion of the IMA, and divides initially into two main branches, one supplying the left side and one the right of the upper portion of the rectum. The middle and inferior rectal branches on the other hand, have paired origins, one arising from the left internal iliac and the other from the right internal iliac artery.
Applied Anatomy |
 SMA
SMA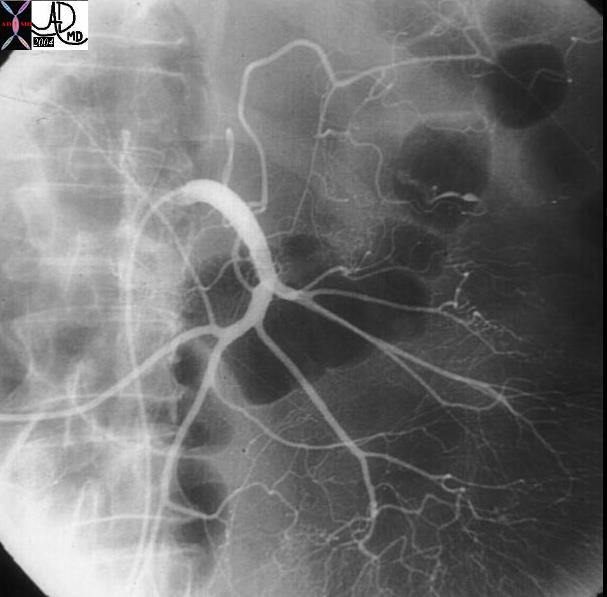
 Colonic supply from the SMA
Colonic supply from the SMA Coronal CT
Coronal CT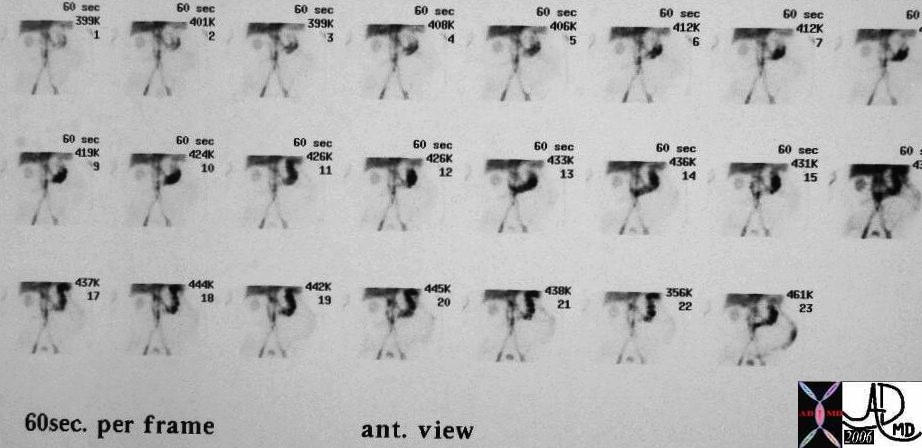 Labelled red cell scan
Labelled red cell scan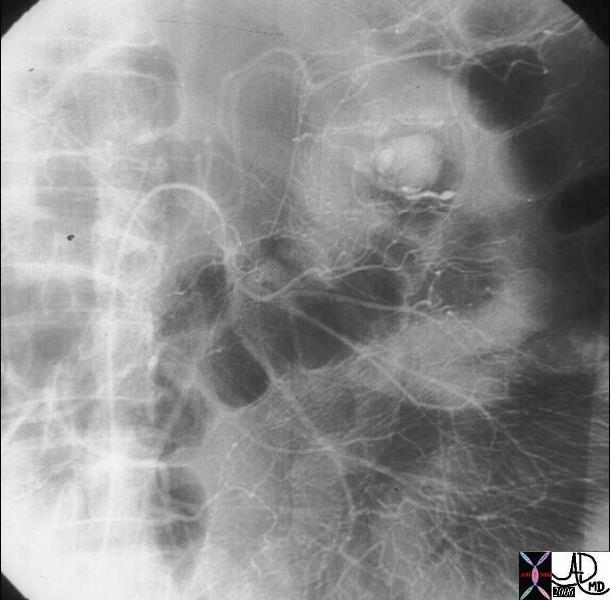
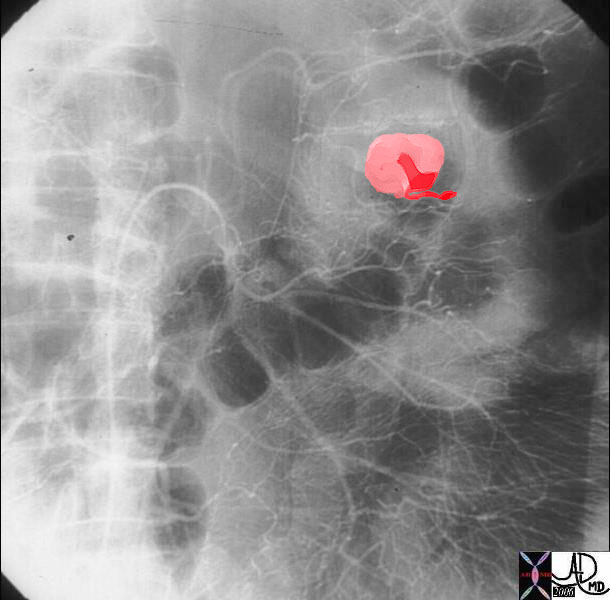 Bleeding artery of the splenic flexure.
Bleeding artery of the splenic flexure.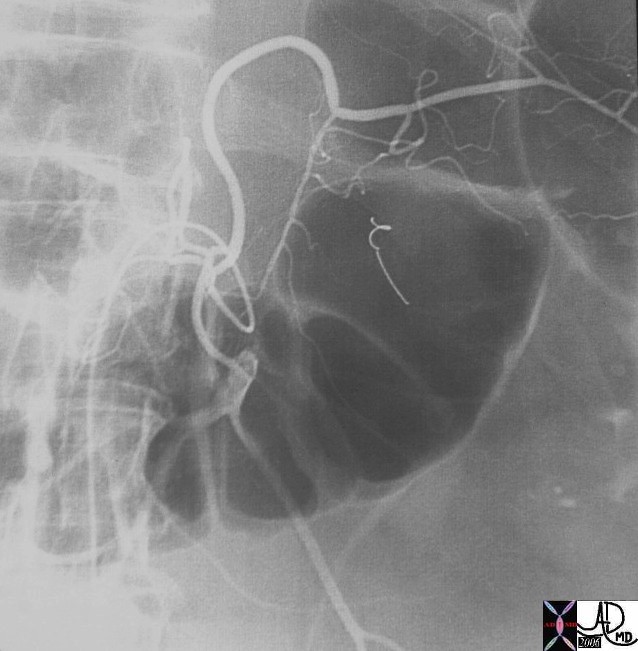 Fig 1
Fig 1
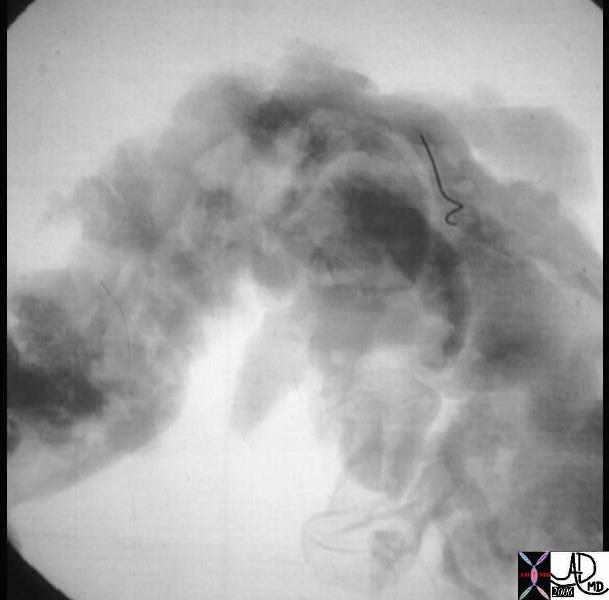 Fig 2
Fig 2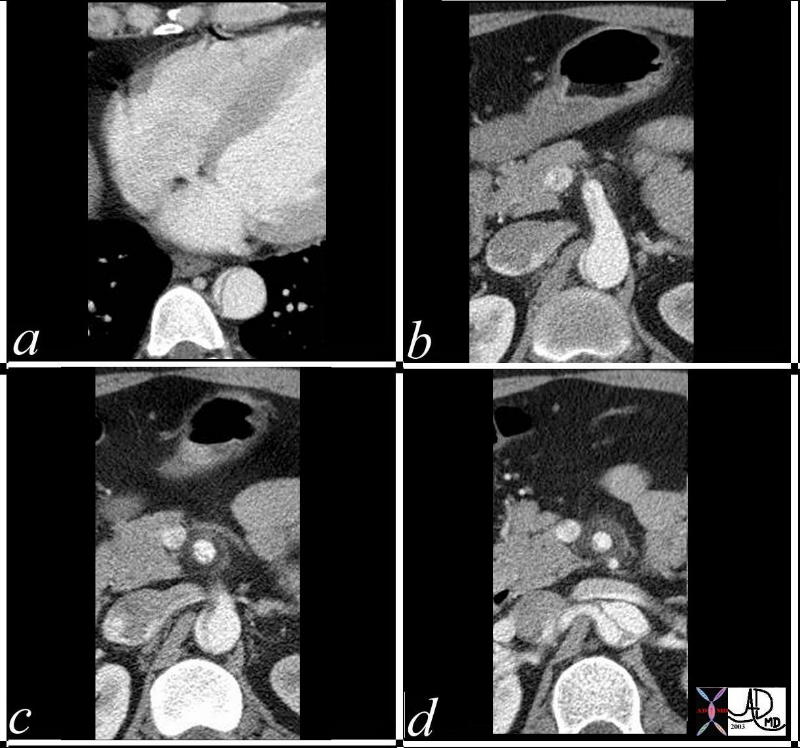 SMA dissection
SMA dissection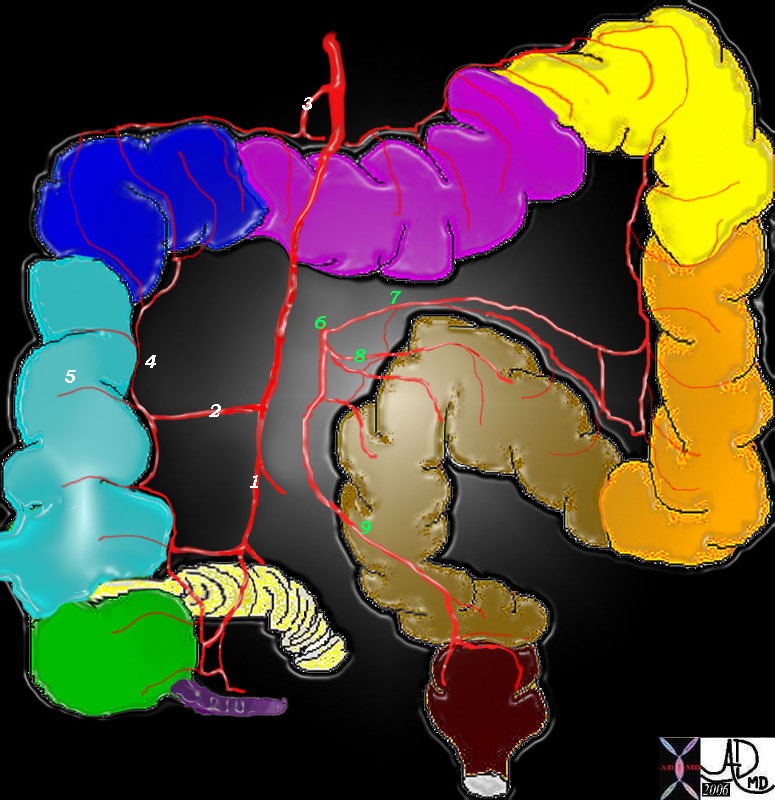 IMA
IMA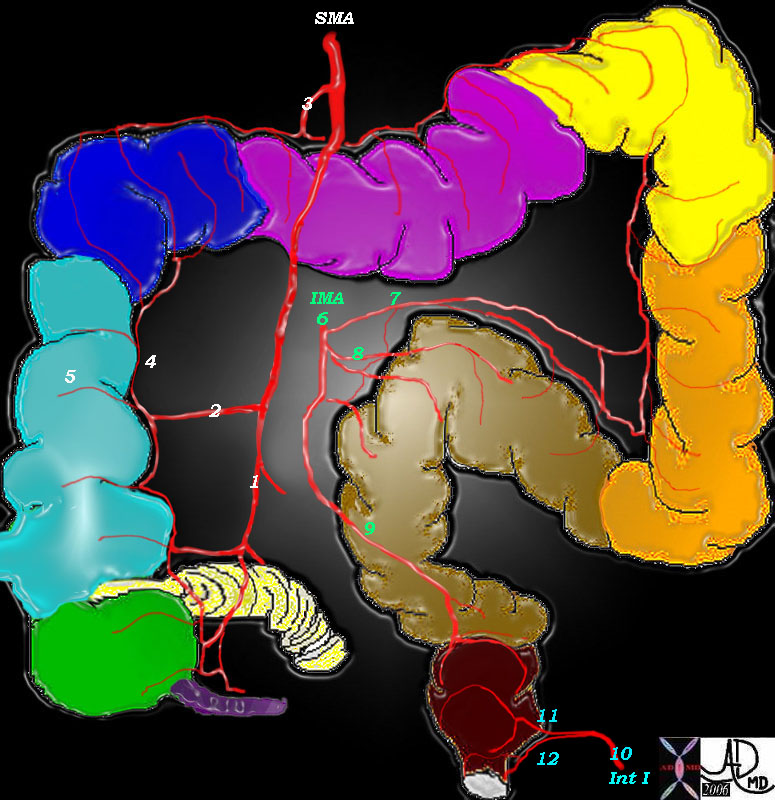
 Collateral and connections of the mesenteric circulation Collateral and connections of the mesenteric circulation |
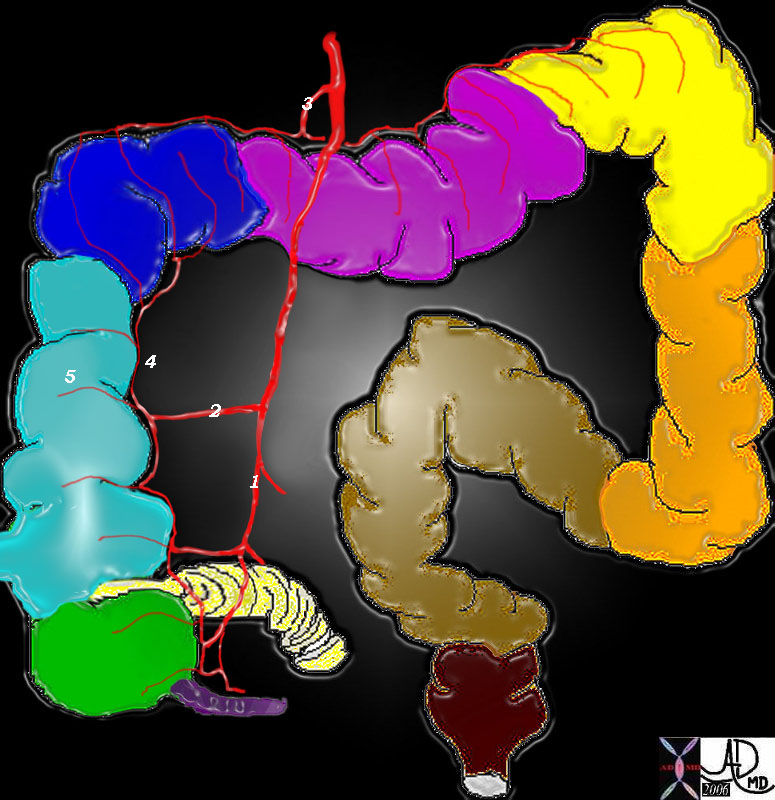
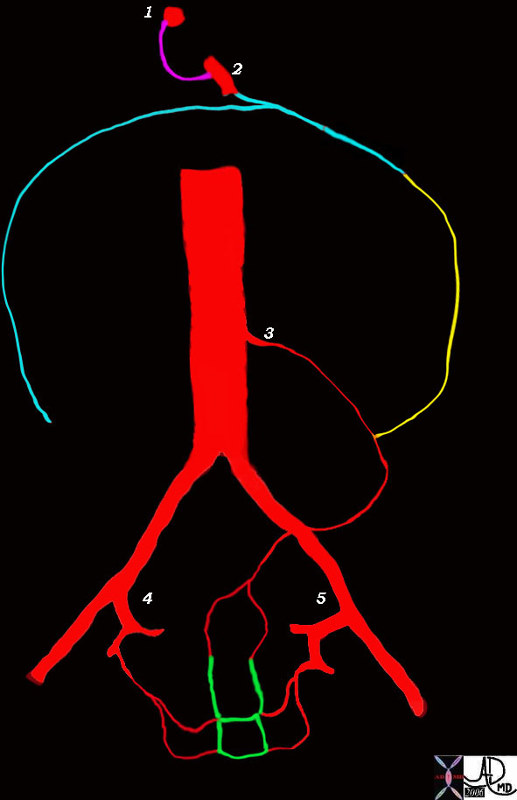
| The diagram represents the circulation of the intestinal tract with the collateral connections between the foregut vessel the celiac axis (1), the midgut vessel, the SMA, and the hindgut vessels – IMA (3), right internal iliac (4) and left internal iliac (5). The connections between the celiac axis and SMA are via the pancreaticoduodenal arcade and transverse pancreatic artery (pink). The contribution of the SMA to the SMA-IMA connections is via the middle colic and marginal arteries (teal), while the IMA contribution to the SMA-IMA connection is also via the marginal artery but on the left side (yellow). The connections between the mesenteric circulation and the systemic circulation are via collateral connections between all the rectal arteries and the internal iliac arteries. The rectal branches have extensive connections which collateralize both supero-inferiorly and from left to right side as well (green).
Courtesy Ashley Davidoff 45581b05 |
In the case of severe stenosis or occlusion of the common the IMA via the superior circulation will help support the vessels to the legs, and will connect to the distal rectal circulation and then via the internal iliac to the external iliac distal to the upstream stenosis or obstruction.
  Acute dissection of the IMA Acute dissection of the IMA |
|
|
Because the rectum has such a rich blood supply as previously stated it is rarely involved in ischemic changes. Thus as in the following patient, if the rectum is involved with an inflammatory process it is unlikely to be ischemic in origin.
 Rectal disease Rectal disease |
||
|
————–
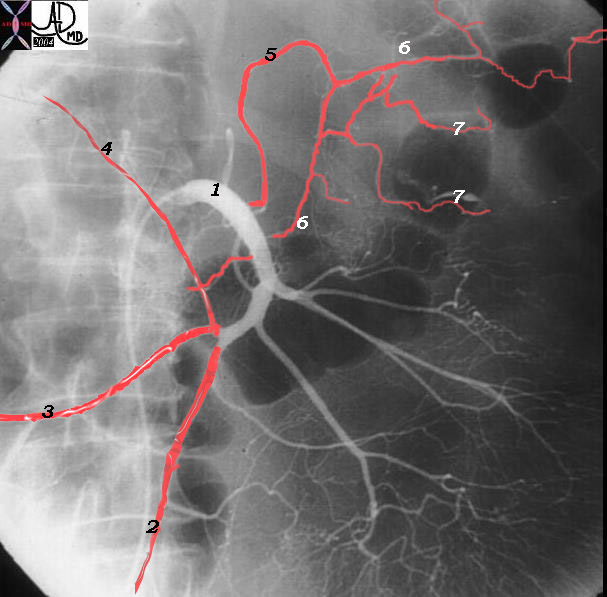
  IMA IMA |
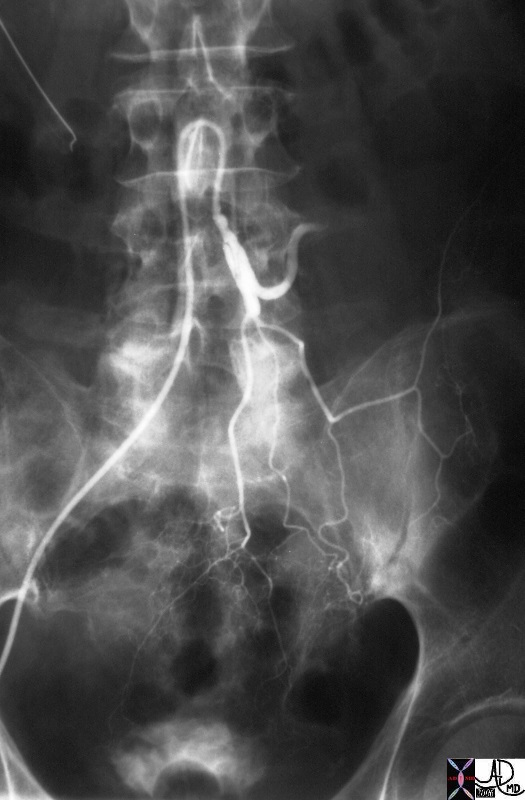
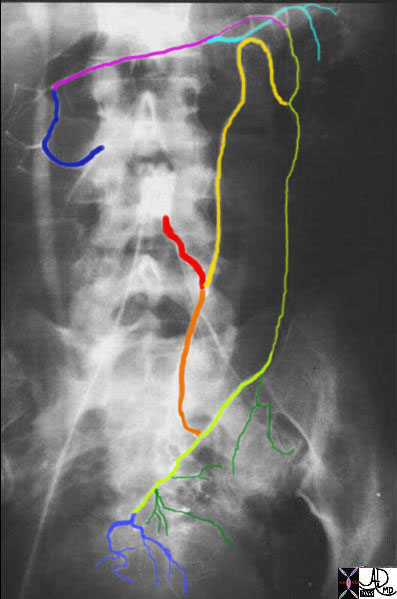
| The IMA (red) gives rise to the left colic artery which divides into an ascending branch (yellow) and a descending branch (orange) both contributing to the left sided marginal artery. (lime green). In the pelvis the marginal artery gives rise to three sigmoid branches (dark green) and the superior rectal artery (dark blue) At the splenic flexure the marginal artery from the left colon (lime green) links to the marginal artery supplied by the left branch of the middle colic artery. (pink). The light blue vessel in the left upper quadrant is a vasa recta vessel from the pink marginal and the dark blue vessel superiorly is the origin of the middle colic artery.
Courtesy Ashley Davidoff MD 12006 12006b |
  Rectal Circulation Rectal Circulation |
| The injection of contrast into the IMA shows the left sided component of the superior rectal artery (bright red) and retrograde filling of the middle rectal and inferior rectal arteries (maroon) supplied by the right internal iliac artery.
Courtesy Ashley Davidoff MD 12020 12020b02 |