|
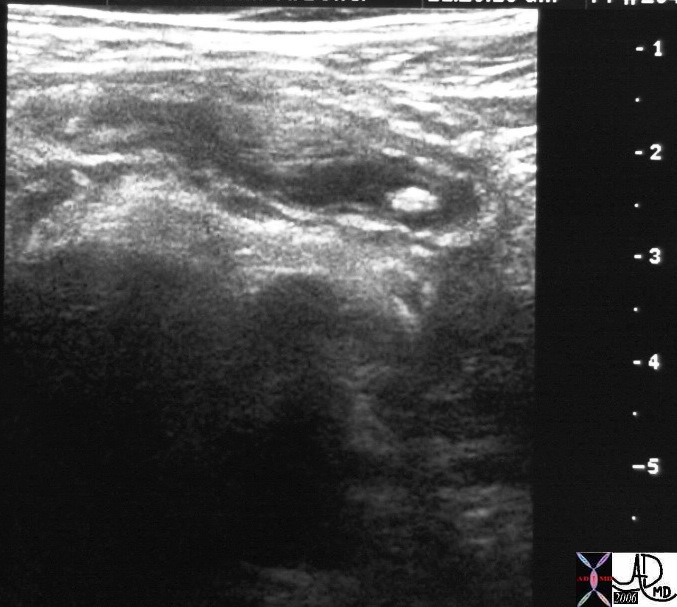
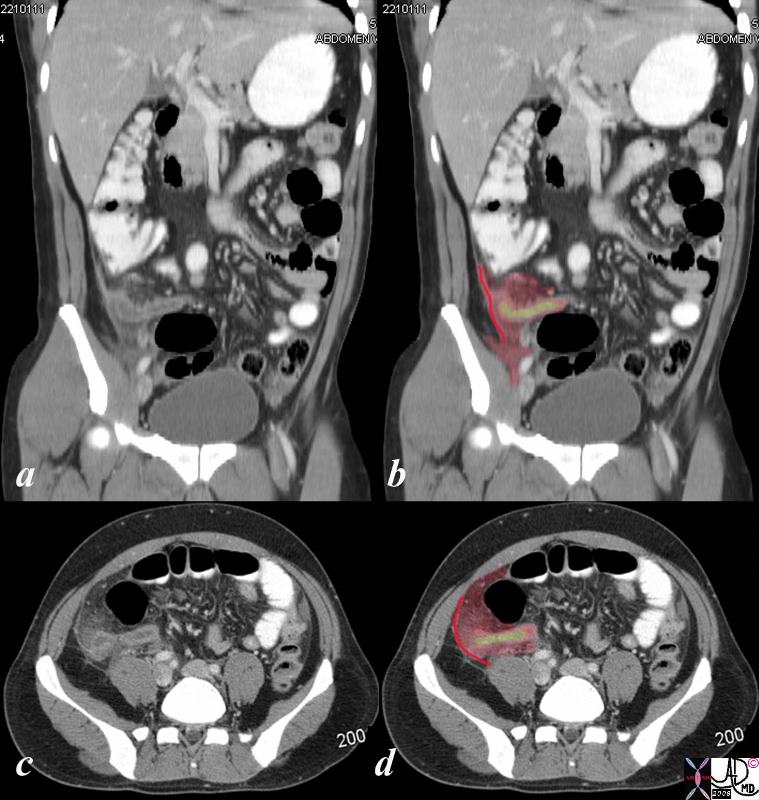
The Common Vein Copyright 2010 Section Name Appendicitis is an inflammatory condition of the appendix caused primarily by an initial obstruction with secondary infection, distension, and subsequent infarction and rupture. The appendix is a long tube-like structure (diverticulum) which extends from the cecum. The obstruction may be caused by lymphoid hyperplasia (often related to a viral illness), foreign bodies and fecoliths, or related to Crohn’s disease. Acute appendicitis is the most common surgical emergency in the Western World. It typically affects teenagers and young adults, though may occur in younger children and infants. There is a smaller secondary peak in the elderly. Structural considerations The appendix is situated in the right lower quadrant but its origin off the cecum is quite variable so that it may be anterior, medial or posterior to the cecum. its length also varies, so for example a very long retrocecal appendix may reach to the right upper quadrant. Depending on the anatomic location of the appendix, it may be initially difficult to differentiate from other causes of acute pelvic pain Clinically, appendicitis classically presents with abdominal pain that starts at the umbilicus and and migrates to the right lower quadrant . It is usually associated with systemic symptoms and signs such as nausea, vomiting, fever. The pain almost always precedes the vomiting. On examination there is usually tenderness with guarding and rebound in the right lower quadrant at Mc Burney’s point, and rectal examination usually reveals right sided pelvic tenderness. Systemically mild dehydration, fever and an elevated wcc are associated signs. (Family Practice Notebook). The classical pain only occurs in about 50% of patients. When the patients presents with these classical features there is no reason to go any further with imaging to confirm the diagnosis. However appendicitis is notoriously a masquerader from being relatively asymptomatic to having severe visceral and somatic pain. When clinical findings are equivocal diagnostic imaging choices include ultrasound and CTscan are considered. In children, and young thin females, ultrasound is the study of choice. Ultrasound is extremely dependant on the opearator, and also is made difficult if bowel gas is present. In the older population, CT is preferred. The overall accuracy of US for appendicitis is reported at 70-95% and for CT accuracy is 93-98%. CT is indicated when perforation or peritonitis is clinically suspected. Treatment is surgical. Laparoscopic removal is frequently utilized. Sometimes, open laparotomy is required, such as when an associated abscess is suspected.
|